Surgery Videos

Ingrown Toenail

Lap Band Procedure done on a patient with a BMI of 45. Minimal editing and includes narration.

Laparoscopy in acute bowel obstruction following previous surgery is a difficult procedure and avoided by most of the surgeons due to the difficulty in obtaining pneumoperitoneum, port placement, lack of working space, adhesions and risk of bowel injury.
Here is a patient who had a previous laparotomy for trauma with a midline incision from xyphysternum to pubis; after unsuccessful conservative management he underwent a laparoscopy; a prior CT scan showed adhesions in the left side and a distal-mid small bowel obstruction. The pneumoperitoneum was obtained with the Visiport placed in the right lower quadrant; although the abdomen was grossly distended, under significant tension and distended loops of small bowel were occupying most the peritoneal cavity, with muscle relaxation there is usually enough space to perform a thorough inspection of the abdominal cavity. Port placement has to be done with special care as there is no room to push and usually a blunt trocar directed away from the bowel is employed in my practice. The collapsed loops of small bowel point quickly to the site of obstruction -- it is better to avoid manipulating the distended bowel as it is heavy, oedematous and prone to be lacerated with the instruments; once the pathology is identified, in this case the obstructive band, light packing is performed in order to expose the working space and protect the bowel from instruments like scissors or diathermy. In this case the band adhesion was slightly more difficult to separate from the bowel and required a combination of sharp and gentle blunt dissection.
Once the obstruction is release and the transit of contents is confirmed in the collapsed bowel the procedure is terminated. No abdominal drainage is usually necessary.

Giant spigelian stranguled hernia with small bowel loop and omental flap inside. The omentum required resection, the bowel appears vital. After the handle of hernia sac and his content has been done, a overlapped prolene repair will be done.

Right indirect (Gilbert II)inguinal hernia has been repared using PHSe prosthetic device

A posterior Gastroenteral side to side anastomosis is presented. The procedure is made with circular stapler. After a good hemostasis of the suture has been obtained, the gastrotony is closed with linear stapler and running suture.

Repair of the umbilical hernia, and placing the omentum back in

19 years old young man with inguinoscrotal right hernia.Decision-making for repair with minimal prosthetic residual material, and no stitches use for best comfort

Open Appendectomy Surgery Video

The operation was done by cut opening the abdomen for resection anastamoses of intestine. You can see all intestines. The patient unfortunately died of sepsis. He was just 15 yrs old

Appendectomy operation

Intussuseption and Appendectomy
Splenectomy for a giant spleen
This shows a full Abdominoplasty surgery performed by Dr. Art Foley in Olympia Washington. Abdominoplasty is also commonly referred to as a "Tummy Tuck." Tummy tuck is a surgical procedure also known as abdominoplasty to remove excess skin and fat from the middle and lower abdomen and to tighten the muscles of the abdominal wall. The procedure can dramatically reduce the appearance of a protruding abdomen. But bear in mind, it does produce a permanent scar.
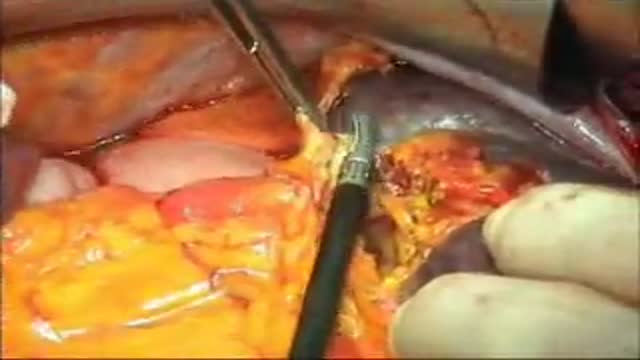
Modern technique of thyroidectomy for tumors

Fibroma Excision in the Cheek

Removal of the superficial lobe is performed on a child presenting with a mass

parotidectomy has always been considered to be a daunting aesthetic surgical exercise reuiring extreme care to safeguard the facial nerve. most surgeons master the skill with experience and effort and develop thier own tips and tricks for safe conduct of the procedure. details of the procedure along... with practical tips are illustrated in the video for the benefit of head neck surgeons

TRAM only in cases where a Diep or Gracilis is not applicable

En Bloc Esophageal Mucosectomy, an experimental technique for the endolumenal management of Barrett's related dysplasia and neoplasia. High grade dysplasia is in indication for esophagectomy; however esophagectomy has a mortality rate up to 12 percent, and up to 56 percent of patients may develop s...erious post-operative complications. Multiple ablated lesions can progress under the neo-squamous layer, leading to buried Barrett's mucosa. With conventional piecemeal EMR, cautery effect limits evaluation in areas of interest, Barrett's epithelium is left behind, tissue is not evaluated in situ and invasive lesions may be missed due to incomplete sampling. A new technique, en bloc esophageal mucosectomy, or EEM, was developed. The technique begins with conventional EMR in the proximal esophagus to access the submucosal space. Conventional EMR is being performed here. The mucosa is resected using an electrothermal snare. The mucosal defect from the first EMR is seen here. EMR is then repeated on the opposing wall. Sequential EMR creates a complete concentric mucosal defect. In the following sequence the completely detached column of mucosa can be seen, bounded by submucosa and muscularis propria layers. Here in the stomach, the endoscope is retroflexed and is covered by a sleeve of esophageal mucosa which has been freed to the GE junction and inverted. This sequence demonstrates a double snare technique. This snare is alongside the endoscope. The snare has been passed through the working channel. The working channel snare is pulled back, and the snare alongside the scope is used to grasp the mucosal column. With tension on the column the working channel snare can be threatened and advanced. This sequence shows the snare as it is being passed down to the GE junction. At the GE junction, the snare is tightened and cautery is applied. This frees the column of mucosal tissue from the remaining attachment. The endoscope is then withdrawn. Then detached mucosal column can be grasped with a snare and retrieved. In the following sequence, the long column of mucosa is being withdrawn via the overtube. Here, endoscopic forceps have been passed through the column to demonstrates the concentric nature of the specimen. The length of mucosa can be seen here alongside 2 conventional EMR specimens. Approximately 15cm of tissues was removed in this case. On endoscopy immediately following the resection, there is no bleeding or evidence of perforation in the area of resection. The endoscope is advanced and the exposed submucosa can be appreciated down to the GE junction. This is the low power view of the histologic specimen generated by EEM. Metaplastic tissue adjacent to a dysplastic focus would be completely removed. With a high power view, the layers of the esophagus can be appreciated. The epithelium, lamina propria, muscularis mucosa and submucosa are visible, with no cautery artifact in the area of interest. The technique would remove metplasia, low grade dysplasia, high grade dysplasia, and intramucosal carcinoma, as well a T 1 a lesions. All the animals in this series tolerated the procedure well. A total of five non-survival procedures and 4 survival procedures were performed. In the survival procedures, all four swine thrived in the post-operative period. Two swine were then survived for 9 days following the procedure. On post —op day nine, after passing into the upper esophagus, the proximal margin of the mucosectomy is seen here. Healing appears to be occurring. There is no evidence of leak, and no stricting is seen at 9 days down to the GE junction Passing into the stomach, some residual feed can be seen. Two swine were then survived for 13 days. On this follow-up endoscopy, the area of the mucosectomy is again healing. There was a loose stricture in both animals and both were easily traversed with a 9.8 mm gastroscope. There was a gross appearance of re-epitheliazation in some areas. It is notable that the stricture was present in the proximal esophagus with no narrowing distally. At necropsy there was not eviden
