Plastic Surgery

http://www.rhinoplastyspecialist.com
One of the most common of all plastic surgery procedures is rhinoplasty, also commonly known as a nose job. Rhinoplasty surgery can serve dual purposes, creating a more aesthetically pleasing look and also helping breathing conditions, such as a deviated septum.. Whether it's because of a genetic defect or some kind of injury, many people have trouble breathing through their nose. A rhinoplasty can counteract this, clearing the airway so you can breathe freely. It can even repair a deviated septum, straightening it and removing any blockages in the airway.
Perfecting surgery with this three-dimensional structure (the nose) takes years to master and continues to improve. Little did we know that rhinoplasty maneuvers that were used three years ago could cause disastrous results today. Rhinoplasty surgery is forever evolving! My fellowship director, J. Regan Thomas, MD, told me something that I’ll never forget – “you haven’t learned anything about rhinoplasty until you’ve performed at least a thousand procedures and followed them for many years”. This statement epitomizes why fellowships are so valuable. Some of the needed experience and potential pitfalls are circumvented by first hand observing and learning the analysis, judgment, techniques, complication management and most importantly, results from a seasoned rhinoplasty surgeon. This is why I super-specialized in rhinoplasty surgery during my fellowship in Facial Plastic & Reconstructive Surgery. The training catapults you years ahead of many other surgeons that aren’t fortunate to have post-graduate training. Many cosmetic surgeons are taught that aggressive cartilage removal is a procedure of the past. Today’s concept is “less is more”. Less cartilage excision, cartilage repositioning, camouflage techniques, structural grafting and suturing techniques are being taught in most rhinoplasty courses and at our national meetings.
http://www.rhinoplastyspecialist.com
120 S. Spalding Drive Suite 315 Beverly Hills, CA 90212 Tel: (310)-275-2467

avara plastic surgery center in Cairo Egypt where you can have amazing excellent surgery with very competitive price and at the same time spend your marvelous vacation in charming red sea
مركز افارا لجراحات التجميل في مصر هو مركز متخصص في جراحة التجميل بكافة فروعها تصغير المؤخرة تصغير الارداف تنسيق القوام شد المؤخرة و جراحة الثدي تكبير الثدي تكبير الصدر تجميل الثدي تجميل الصدر شد الثدي شد الصدر تصغير الثدي تصغير الصدر رفع الثدي رفع الصدر شد الترهلات شد الجسم شد البطن شد الارداف شد المؤخرة رفع المؤخرة تجميل الانف تصغير الانف زراعة الشعر شد الجفون تجميل الجفن تجميل العين شد الوجة تجميل الاذن شفط الدهون شفط الشحوم بالليزر تصغير الساق نحت الجسم ازالة الشعر بالليزر علاج الهالات السوداء تجميل الوجة تجميل البشرة تجميل الجسم بدون جراحة حقن الدهون نفخ الوجة حقن السيايكون جقن الفيليرز حقن البوتكس علاج تجاعيد الوجة تقوية الشعر تكبير الخدود تكبير الشفايف

Breast reconstruction 3D Animation
on Friday, December 17, 2010
The primary part of the procedure can often be carried out immediately following the mastectomy. As with many other surgeries, patients with significant medical comorbidities (high blood pressure, obesity, diabetes) and smokers are higher-risk candidates. Surgeons may choose to perform delayed reconstruction to decrease this risk. Patients expected to receive external beam radiation as part of their adjuvant treatment are also commonly considered for delayed autologous reconstruction due to significantly higher complication rates with tissue expander-implant techniques in those patients. Breast reconstruction is a large undertaking that usually takes multiple operations. Sometimes these follow-up surgeries are spread out over weeks or months. If an implant is used, the individual runs the same risks and complications as those who use them for breast augmentation but has higher rates of capsular contracture (tightening or hardening of the scar tissue around the implant) and revisional surgeries. Outcomes based research on quality of life improvements and psychosocial benefits associated with breast reconstruction served as the stimulus in the United States for the 1998 Women's Health and Cancer Rights Act which mandated health care payer coverage for breast and nipple reconstruction, contralateral procedures to achieve symmetry, and treatment for the sequelae of mastectomy. This was followed in 2001 by additional legislation imposing penalties on noncompliant insurers. Similar provisions for coverage exist in most countries worldwide through national health care programs. There are many methods for breast reconstruction. The two most common are: * Tissue Expander - Breast implants This is the most common technique used in worldwide. The surgeon inserts a tissue expander, a temporary silastic implant, beneath a pocket under the pectoralis major muscle of the chest wall. The pectoral muscles may be released along its inferior edge to allow a larger, more supple pocket for the expander at the expense of thinner lower pole soft tissue coverage. The use of acellular human or animal dermal grafts have been described as an onlay patch to increase coverage of the implant when the pectoral muscle is released, which purports to improve both functional and aesthtic outcomes of implant-expander breast reconstruction. o In a process that can take weeks or months, saline solution is percutaneously injected to progressively expand the overlaying tissue. Once the expander has reached an acceptable size, it may be removed and replaced with a more permanent implant. Reconstruction of the areola and nipple are usually performed in a separate operation after the skin has stretched to its final size. * Flap reconstruction The second most common procedure uses tissue from other parts of the patient's body, such as the back, buttocks, thigh or abdomen. This procedure may be performed by leaving the donor tissue connected to the original site to retain its blood supply (the vessels are tunnelled beneath the skin surface to the new site) or it may be cut off and new blood supply may be connected. o The latissimus dorsi muscle flap is the donor tissue available on the back. It is a large flat muscle which can be employed without significant loss of function. It can be moved into the breast defect still attached to its blood supply under the arm pit (axilla). A latissimus flap is usually used to recruit soft-tissue coverage over an underlying implant. Enough volume can be recruited occasionally to reconstruct small breasts without an implant. o Abdominal flaps The abdominal flap for breast reconstruction is the TRAM flap or its technically distinct variants of microvascular "perforator flaps" like the DIEP/SIEP flaps. Both use the abdominal tissue between the umbilicus and the
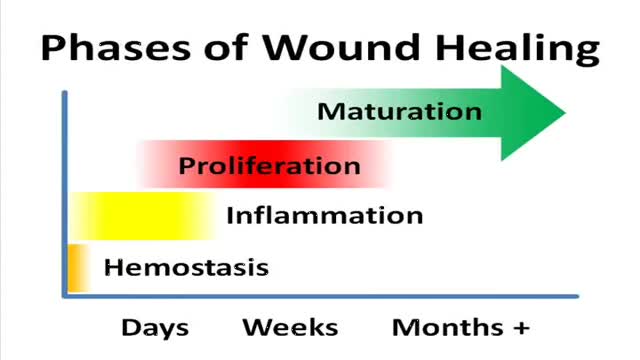
A video showing the phases of normal wound healing

A video showing breast examination after breast implants

Dr. Lin Testimonial 1
Breast Reduction Surgery video Operation مركز افارا لجراحات التجميل الخدود تكبير الشفايف
Nice surgery video
Eye Lid Plastic Surgery in Egypt video

Showing a surgery of re-attaching a hand that was cut away

Otto Placik MD. a board certified Chicago Illinois based plastic surgeon presents instructional video on post genital surgery (labia minora reduction aka labiaplasty or labioplasty or clitoral hood reduction) massage exercises for treatment of labum minora psot surgical fibrosis or hypersensitivity. Photos pictures and video of anatomic models are reviewed . Great for patients thinking about or planning labiaplasty or vaginal cosmetic surgery

Breast augmentation usually is performed in subglandular, subfascial, or partial submuscular pockets, including the dual plane. A new pocket has been described and used by the author. Methods: From October 2005 to April 2008, 600 patients underwent bilateral breast augme...
ntation using the new technique. Soft cohesive gel micro-textured round implants (range 200- 500cc) were used. The initial pocket is made in the subglandular plane up to the lower level of the nipple areolar complex. The submuscular plane is reached by splitting the pectoralis major muscle at the level of middle and lower third of sternum. The muscle is split along the direction of its fibers up and laterally to the anterior axillary fold. No pectoralis major is released from costal margin. The implant lies in this plane simultaneously behind and in front of the pectoralis major. Procedure is performed as a day case under general anesthetic with no drains. Results: Postoperative analgesia requirements is reduced because of dissection in natural planes resulting in quick recovery. No muscle contraction associated deformities is seen. All patients had aesthetically natural cleavage, with the nipple at the most projected part of the breast with three-dimensional enhancement. Conclusion: An adequate muscle cover of the prosthesis is achieved by muscle splitting breast augmentation technique and the procedure is used in all breast augmentations procedures
Tummy Tuck Surgery Video

This a very interesting video showing liposuction and tummy tuck surgery video

Liposuction, also known as lipoplasty (”fat modeling”), liposculpture suction lipectomy or simply lipo (”suction-assisted fat removal”) is a cosmetic surgery operation that removes fat from many different sites on the human body. Areas affected can range from the abdomen, thighs, buttocks, to the neck, backs of the arms and elsewhere.
Suction-assisted lipectomy of bilateral outer thighs
Several factors limit the amount of fat that can be safely removed in one session. Ultimately, the operating physician and the patient make the decision. There are negative aspects to removing too much fat. Unusual “lumpiness” and/or “dents” in the skin can be seen in those patients “over-suctioned”. The more fat removed, the higher the surgical risk.
While reports of people removing 50 pounds (22.7 kg) of fat has been claimed, the contouring possible with liposuction may cause the appearance of weight loss to be greater than the actual amount of fat removed. The procedure may be performed under general or local (”tumescent”) anesthesia. The safety of the technique relates not only to the amount of tissue removed, but to the choice of anesthetic and the patient’s overall health. It is ideal for the patient to be as fit as possible before the procedure and not to have smoked for several months.

DMC Pediatric Plastic and Reconstructive Surgeon Dr Arlene Rozzelle and her team of specialists repair a newborn’s cleft lip.

Dr. Thomas Haas, MD, Board Certified plastic surgeon, performed breast augmentation on his patient in November, 2007. The surgery was performed in his JCAHO accredited in-office Surgery Suite (Imaage) located in Louisville, Kentucky. With so many women interested in this surgery, this video can answer many of their questions. Dr. Haas specializes in cosmetic and aesthetic surgery and has been in practice over 15 years

تكبير الثدي تكبير الصدر تجميل الثدي تجميل الصدر

Bat Ears Correction Plastic Surgery

Closed Rhinioplasty Exposing The Nasal Structures
