Urology

Endoscopic crushing of a bladder stone very interesting medical video

A DMC patient with urinary stress incontinence regains control with less-invasive surgery at DMC Sinai-Grace, performed by DMC Ob/Gyn specialist Dr. Korial Atty. ~ Detroit Medical Center

Urethroplasty is a surgical procedure to correct scar tissue blockage of the urethra called urethral stricture. ~ Detroit Medical Center

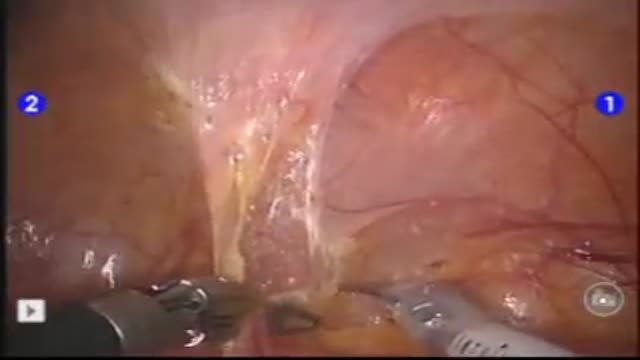
Laparoscopic repair in rupture of urinary bladder

Distal Urethroplasty with Dorsal Dartos Flap

Proximal Hypospadias repaired by Tube Onaly Urethroplasty

How diabetes effects the kidneys.
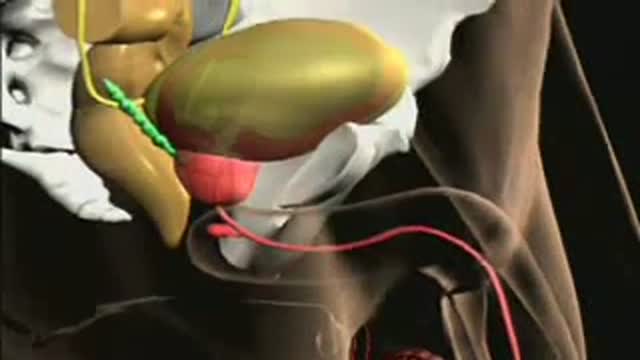
Anatomy of the Prostate
PURPOSE: Laparoscopic partial nephrectomy (LPN) is an alternative modality of treatment for small sized renal cell carcinoma. Robot assisted laparoscopic partial nephrectomy (RLPN) has also been performed with an advantage in repairing resected surface after tumor resection. We compare the periopera...
tive data of patients treated with laparoscopic partial nephrectomy with those of RLPN undertaken patients. MATERIAL AND METHOD: From September 2006 to April 2008, 22 patients were treated with LPN and 22 were RLPN. 3 arms were used for RLPN; camera was inserted through the 12mm, umbilical trocar port. The laparoscopic Bulldog clamp was used for the clamping of renal hilum. We retrospectively compared each group about tumor size, operation time, estimated blood loss, warm ischemic time and hospital stay. RESULT: Operation time of LPN was shorter than that of RLPN (p=0.033). Tumor size, estimated blood loss and hospital stay was not significant different in each group. No case had conversion to open surgery. 1 patient of RLPN group, however, had conversion to radical nephrectomy due to severe bleeding. CONCLUSION: RLPN was safe and feasible in small sized renal cell carcinoma. Warm ischemic time was reasonable and morbidity associated with RLPN was also low. RLPN LPN p-value Tumor Size (cm) 2.5 2.1 0.605 Op time (min) 169.3 140.8 0.033 EBL (ml) 243.2 213.2 0.878 Warm Ischemic Time (min) 29.2 26.4 0.237 Transfusion (%) 4.5 4.5 0.756 Hospital stay (day) 4.4 5.5 0.053

51 yr old female with right flank pain and recurrent UTI. IVP showed a UPJ calculus on the right.

No Scalpel Vasectomy
Urogenital neoplasms spreading to the inguinal lymph nodes are penile carcinoma (the most frequent), urethral and scrotum cancers, tumors of the testis with scrotal violation. Penile carcinoma is an uncommon malignant disease and accounts for as many 0.4-0.6% of male cancers. Most patients are elder...ly. It rarely occurs in men under age 60 and its incidence increases progressively until it reaches a peak in the eighth decade 1. The risk of a lymph node invasion is greater with high grade and high stage tumors 2. Some investigators have reported the inaccuracy of the sentinel node biopsy 3, 4, described by Cabanas 5. Patients with metastatic lymph node penis cancer have a very poor prognosis if penectomy only is performed. Ilioinguinal lymphadenectomy is basically carried out as a treatment modality and not only as a staging act. Patients with lymph node invasion have a 30-40% cure rate. Ilioinguinal lymphadenectomy should be also performed in patients with disseminated neoplasms for the local control of the disease. The 5 years survival rate of patients with clinically negative lymph nodes treated with a modified inguinal lymphadenectomy is 88% versus 38% in patients not initially treated with lymphadenectomy 6. This video-tape clearly shows a therapeutic algorithm, the anatomy of the inguinal lymph nodes, according to Rouviere 7 and Daseler 8, the radical ilioinguinal node dissection with transposition of the sartorius muscle and the modified inguinal lymphadenectomy proposed by Catalona 9. References: 1. Lynch D.F. and Schellhammer P: Tumors of the penis. In Campbell’s Urology Seventh Edition, edited by Walsh P.C., Retik A.B., Darracott Vaughan E. and Wein A.J. W.B. Saunders Company, Vol. 3, chapt. 79, p. 2458, 1998. 2. Pizzocaro G., Piva L., Bandieramonte G., Tana S. Up-to-date management of carcinoma of the penis. Eur. Urol. 32: 5-15, 1997 3. Perinetti E., Crane D.B. and Catalona W.J. Unreliability of sentinel lymph node biopsy for staging penile carcinoma. J. Urol. 124: 734, 1980 4. Fowler J.E. Jr. Sentinel lymph node biopsy for staging penile cancer. Urology 23: 352, 1984 5. Cabanas R.M. An approach for the treatment of penile carcinoma. Cancer 39: 456, 1977 6. Russo P. and Gaudin P. Management strategies for carcinoma of the penis. Contemporary Urology;5:48-66, 2000 7. Rouviere H. Anatomy of the human lymphatic system. Edwards Brothers, p. 218, 1938 8. Daseler E.H., Anson B.J., Reimann A.F. Radical excision of the inguinal and iliac lymph glands: a study based on 450 anatomical dissections and upon supportive clinical observations. Surg. Gynecol. Obstet. 87: 679, 1948 9. Catalona W.J. Modified inguinal lymphadenectomy for carcinoma of the penis with preservation of saphenous veins: technique and preliminary results. J. Urol. 140: 306-310, 1988

McMaster University technique of Laparoscopic Radical Nephrectomy

Robotic Prostatectomy: Cornell Athermal Robotic Technique
