- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Ophthalmology

Eye Pressure Test
Contact Lens Safety and complications


Corneal cross-linking (CXL) is an in-office eye procedure that strengthens the cornea if it's been weakened by keratoconus, other corneal disease, or (rarely) a complication of LASIK surgery. Alternative and brand names for the procedure include corneal cross-linking, corneal collagen cross-linking, C3-R, CCL and KXL.

With keratoconus, the clear, dome-shaped tissue that covers the eye (cornea) thins and bulges outward into a cone shape. Its cause is unknown. Symptoms first appear during puberty or the late teens and include blurred vision and sensitivity to light and glare. Vision can be corrected with glasses or contact lenses early on. Advanced cases may require a cornea transplant.
An eye web is a noncancerous, triangular growth that may occur on one or both eyes. It's more common in people who spend a lot of time in the sun, such as those who work outdoors. The painless growth may be slightly raised and contain obvious blood vessels. It may cause irritation and possibly affect vision. Treatment usually isn't necessary. Eyedrops or surgery may help in severe cases.
LASIK eye procedure for correcting vision

cleral tattooing is the practice of tattooing the sclera, or white part of the human eye. The dye is not injected into the tissue, but between two layers of the eye, where it spreads out over a large area. The process is not common

Retinitis pigmentosa is a rare, inherited degenerative eye disease that causes severe vision impairment. Symptoms often begin in childhood. They include decreased vision at night or in low light and loss of side vision (tunnel vision).
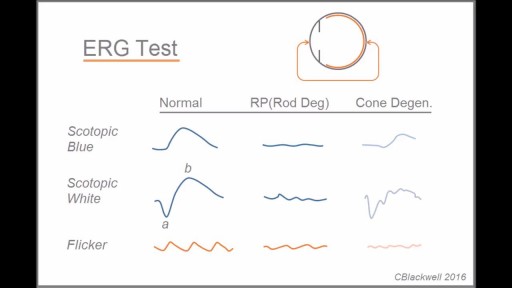
Retinitis pigmentosa is a rare, inherited degenerative eye disease that causes severe vision impairment. Symptoms often begin in childhood. They include decreased vision at night or in low light and loss of side vision (tunnel vision). There's no effective treatment for this condition. Wearing sunglasses may help protect remaining vision.


Blepharoplasty (BLEF-uh-roe-plas-tee) is a type of surgery that repairs droopy eyelids and may involve removing excess skin, muscle and fat. As you age, your eyelids stretch, and the muscles supporting them weaken. As a result, excess fat may gather above and below your eyelids, causing sagging eyebrows, droopy upper lids and bags under your eyes. Besides making you look older, severely sagging skin around your eyes can reduce your side vision (peripheral vision), especially the upper and outer parts of your field of vision. Blepharoplasty can reduce or eliminate these vision problems and make your eyes appear younger and more alert. To help decide if blepharoplasty is right for you, find out what you can realistically expect and explore the benefits and risks of blepharoplasty.


Blepharoplasty

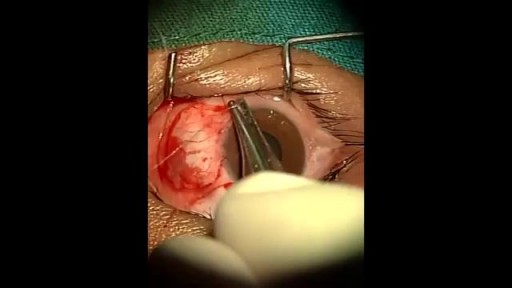
The eyelid is injected with a local anesthetic, a clamp is put on the eyelid, then the eyelid is turned over, an incision is made on the inside of the eyelid, and the chalazion is drained and scraped out with a curette. A scar on the upper lid can cause discomfort as some patients feel the scar as they blink.
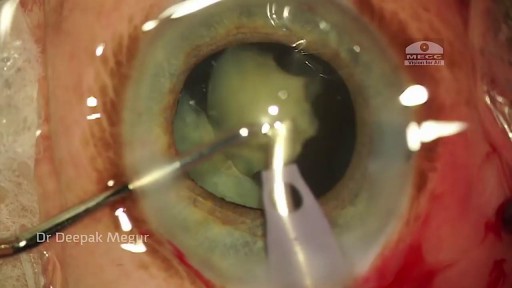
Phacolytic glaucoma usually is associated with a mature or hypermature cataract and typically occurs in elderly patients. Today, phacolytic glaucoma is rare in the United States, found primarily in areas where access to care is poor. Will the increase in the number of under- and uninsured patients lead to an increase in this condition? Evaluation and Diagnosis Signs and symptoms. Patients typically report acute-onset pain, decreased vision, tearing and photophobia. Examination will reveal injection, corneal edema, elevated IOP, anterior chamber reaction with or without pseudohypopyon, particles on the lens capsule and anterior capsule wrinkling. Patient history. The duration of symptoms should be elicited; a delayed presentation of more than five days since onset can result in glaucomatous disc damage and poorer prognosis.¹ The ocular history may reveal that the patient decided against removal of an advanced cataract. Prior intraocular surgery or trauma may have left residual lens material that could cause phacoanaphylactic glaucoma or exacerbate infectious endophthalmitis. Visual acuity and visual potential should be assessed. Exam essentials. A complete ophthalmologic examination should be done. The eye should be inflamed, and the cornea may be edematous due to the high IOP. The anterior chamber will demonstrate massive inflammation and/ or pseudohypopyon. Gonioscopy is essential; it will help rule out angle closure due to phacomorphic glaucoma or neovascularization of the angle. Assess ment of the posterior pole should be performed to rule out vitreous hemorrhage (which can result in ghost-cell glaucoma) or vitritis (which may be associated with infectious endophthalmitis or panuveitis). If the view to the fundus is obstructed, B-scan ultrasonography also should be performed. Differential diagnosis. The differential diagnosis includes infectious endophthalmitis, phacoanaphylactic glaucoma, inflammatory glaucoma, glaucoma secondary to intraocular tumor, phacomorphic glaucoma, acute-angle closure glaucoma and neovascular glaucoma. Management Medication. Medical management is used to temporarily control the glaucoma and inflammation. Initial treatment consists of hyperosmotic agents, aqueous suppressants, anti-inflammatory drugs and cycloplegics. Surgery. Definitive treatment is removal of the lens via extracapsular cataract extraction with or without an IOL. Some ophthalmologists defer placement of an IOL until after the inflammation subsides; however, there is no significant difference in final visual acuity between those patients who did receive an IOL and those who did not.¹ If the phacolytic glaucoma is of long duration (more than seven days), a combined trabeculectomy may be needed to prevent postoperative IOP spikes.² In eyes with hypermature Morgagnian cataracts, one must be especially careful, as the capsule is fragile, the zonules are weak and the view is difficult due to the white, milky cortex. Vision limited to light perception on presentation is not a contraindication to performing cataract extraction. Surgical Tips For a planned extracapsular cataract extraction with a posterior chamber IOL, fashion a superior fornix-based conjunctival flap.³ Make a partial-thickness incision along the sclerolimbal junction superiorly for 120 degrees with a No. 69 blade. Forty-five degrees away, a paracentesis should be done to decompress the eye. The anterior chamber fluid can be withdrawn for analysis, to look for macrophages and high molecular-weight proteins. Inject balanced salt solution in a cannula to wash out any residual particulate matter, then inject Healon or viscoelastic into the anterior chamber. Make an incision entering the anterior chamber at the 12 o’clock position with a keratome. A 26-gauge cystotome mounted on a syringe is then introduced through the 12 o’clock incision and used to puncture the capsular bag. The milky cortex should be aspirated as much as possible, until the nucleus is visible. Withdraw the needle through the keratome incision, then inject Healon through the 12 o’clock incision into the capsular bag. Next, enlarge the corneoscleral keratome incision with curved Westcott scissors to 120 degrees. Perform a partial V-shaped capsulotomy; this can be done either with the cystotome or with an angled Vannas scissors. Place viscoelastic under the nucleus to float the nucleus and sever any adhesions between the nucleus and the capsule. The nuclear portion of the lens can then be removed with an irrigating vectis (lens loop) with or without gentle pressure at the inferior limbus (6 o’clock). Irrigate and aspirate the residual cortex with the Simcoe cannula. Inspect the capsular bag; if it is intact, place a posterior chamber IOL into the bag. Close the incision with several interrupted 10-0 monofilament nylon sutures and reattach the conjunctival flap. Potential Sequelae and Prognosis Postoperatively, the patient should be managed with topical steroids and/or aqueous suppressants and hyperosmotics if necessary. Vitreous opacification behind the posterior capsule occurs in a small percentage of eyes. These vitreous opacities are typically absorbed by one to two weeks postoperatively. IOP usually is controlled without antiglaucoma medications after the cataract removal. A detailed glaucoma evaluation (including repeat gonioscopy to assess for peripheral anterior synechiae, visual field and optic nerve status) should be done to assess the extent of glaucomatous damage. The prognosis is dependent on the duration of elevated IOP, PAS and optic nerve damage. In one study, patients who were older than 60 and whose glaucoma was present for more than five days did significantly worse than a comparison group of younger individuals with shorter disease duration.
