Latest videos
Meningococcal meningitis - causes, features, symptoms and treatment
Indwelling urinary catheters are commonly used in hospitals and can lead to preventable catheter-associated UTI. How can rates of catheter-associated UTI be reduced in hospitals? New research findings are summarized in a new NEJM Quick Take. Learn more at http://nej.md/1WoeHdF SHOW MORE
systemic inflammatory response syndrome (SIRS). This is most likely secondary to sepsis from an infection of the patient's Hickman catheter given the associated skin findings, although culture results are needed to confirm this diagnosis. The patient's low blood pressure is likely secondary to developing septic shock, and he has already appropriately been treated with intravenous fluids. Catheter removal is indicated given his hemodynamic instability. Catheter removal is also indicated in patients with severe sepsis with organ hypoperfusion, endocarditis, suppurative thrombophlebitis, or persistent bacteremia after 72 hours of appropriate antibiotic therapy. Long term catheters should also be removed if culture results are positive for S. aureus, P. aeruginosa, fungi, or mycobacteria.
Learn the SIRS Criteria and how to calculate it. Greater than or equal to 2 or more of the following: Temperature Fever of greater than 38°C (100.4°F) or Less than 36°C (96.8°F) Heart Rate Greater than 90 beats per minute Respiratory Rate Greater than 20 breaths per minute or PaCO2 of less than 32mm Hg White Blood Cell Count Greater than 12,000cells/mm³ or Less than 4,000cells/mm³ or Greater than 10% Bands
-Almost all the cases of occupational transmission of HIV have been due to transmission via exposure to blood and certain body fluids. The body fluids wherein standard precautions have been recommended include semen, vaginal secretions, and any other body fluid containing visible blood. Other standard precautions, according to the Center for Disease Control and Prevention (CDC), also apply to cerebrospinal, peritoneal, pleural, pericardia!, synovial fluid, or any other tissue, even though the epidemiologic data regarding the risk of HIV transmission from these fluids is insufficient. Standard precautions do not apply to urine, sweat, tears, sputum, vomitus, and nasal secretions or feces, as long as there is no gross visible blood. The occupational transmission of HIV has never been documented from the above sources.

-Rapidly progressive weakness of the lower extremities following an upper respiratory infection, accompanied by sensory loss and urinary retention, is characteristic for transverse myelitis.
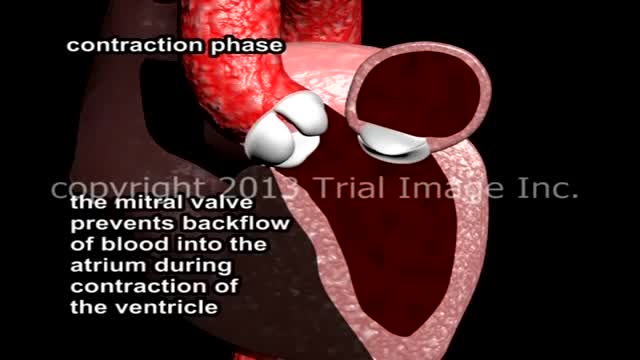
Mitral Valve Prolapse and Mitral Regurgitation. Review of mitral valve anatomy and function, including papillary muscle structure and function, with severe mitral valve prolapse and mitral regurgitation due to a flail segment caused by ruptured papillary muscle and chorda tendinae attachment.
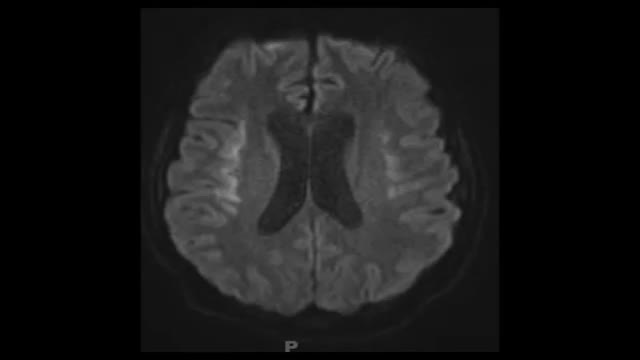
Progressive multifocalleukoencephalopathy is a demyelinating illness of the central nervous system that typically occurs in immunosuppressed patients, especially those with AIDS. It is caused by reactivation of the polyomavirus JC (JC virus) and presents with neurologic deficits including hemiparesis, gait ataxia, visual symptoms, and altered mental status. It is not seen in non-immunosuppressed patients, and fever is not typical
Herpes simplex encephalitis is characterized by acute-onset (<1 week) fever, headaches, seizures, altered mental status, and focal neurologic findings such as hemiparesis or cranial nerve deficits. This patient's weakness/fatigue for >1 week, heart murmur, history of drug abuse, and absence of focal neurologic deficits make endocarditis with mycotic aneurysm more likely than herpes encephalitis
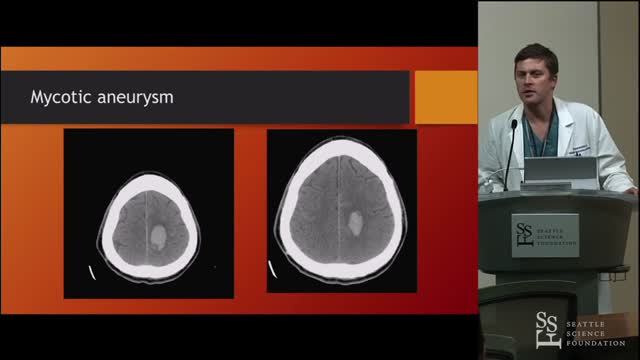
The headache, lethargy, and neck stiffness suggest subarachnoid hemorrhage secondary to rupture of a mycotic aneurysm. Mycotic or infected arterial aneurysms can develop due to metastatic infection from IE, with septic embolization and localized vessel wall destruction in the cerebral (or systemic) circulation. Intracerebral mycotic aneurysms can present as an expanding mass with focal neurologic findings or may not be apparent until aneurysm rupture with stroke or subarachnoid hemorrhage. The diagnosis of mycotic cerebral aneurysm can usually be confirmed with computed tomography angiography. Management includes broad-spectrum antibiotics (tailored to blood culture results) and surgical intervention (open or endovascular).
patient has fever, hypotension, swelling, and erythema of his left leg. Notably, his leg is more painful to palpation than might be expected after visual inspection. These symptoms are very concerning for necrotizing fasciitis. Necrotizing fasciitis is a fulminant infection of the subcutaneous tissue that spreads rapidly along the fascial planes and leads to extensive tissue necrosis and shock. Treatment • Requires surgical debridement & broad-spectrum antibiotics

Two types of clinically distinct necrotizing fasciitis have been described. The most common form (type II) usually occurs in individuals with no concurrent medical illness. Many patients report a history of laceration, blunt trauma, or a surgical procedure as a predisposing factor. It is typically caused by group A Streptococcus (Streptococcus pyogenes). In contrast, type I is usually seen in patients with underlying diabetes and peripheral vascular disease. It is generally a polymicrobial infection; some commonly isolated organisms include Staphylococcus aureus, Bacteroides tragi/is, Escherichia coli, group A Streptococcus, and Pre vote/fa species. Crepitus is more common if anaerobic organisms, such as Clostridium perfringens or 8 tragi/is, are involved.
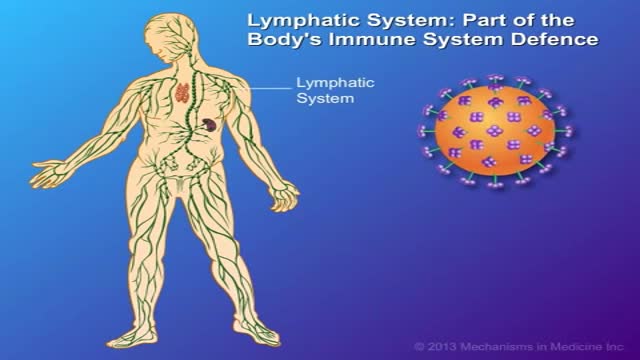
CD4 T-cells (a type of white blood cell) are important to your body's defence against infections. This animation describes how your immune system is weakened by the HIV virus, which targets CD4 T-cells and leads to their gradual decline in number. Low to very low levels of CD4 cells put you at risk for 'opportunistic infections' that take advantage of the body's weakened immune system.
In developing countries, domestic animals (eg, dogs) are common sources of infection. In the United States, bats and wild animals (eg, raccoons) are the most common reservoirs of infection. The acquisition of rabies from bats can occur from an unrecognized bite or a scratch, and possibly by inhalation of aerosolized viral particles. Bats are found in all states except Hawaii, and spelunking (cave exploration) is a risk factor for rabies acquisition from bats.

If you suspect that you have sleep apnea, the usual first step is to discuss your suspicions with your primary care physician. If you don’t have a primary care physician, you can go directly to a clinician who is a sleep specialist. But check your health care insurance coverage first. Some policies require you to see a primary care physician first, and some policies limit the sleep centers and testing facilities whose services they will pay for. Unfortunately, you may discover that your policy offers limited or no coverage for the diagnosis and treatment of sleep apnea, in which case you may wish to switch insurers if and when you can.

Narcolepsy is a chronic sleep disorder characterized by overwhelming daytime drowsiness and sudden attacks of sleep. People with narcolepsy often find it difficult to stay awake for long periods of time, regardless of the circumstances. Narcolepsy can cause serious disruptions in your daily routine. Sometimes, narcolepsy can be accompanied by a sudden loss of muscle tone (cataplexy) that leads to weakness and loss of muscle control. Cataplexy is often triggered by a strong emotion, most commonly laughter. Narcolepsy is a chronic condition for which there's no cure. However, medications and lifestyle changes can help you manage the symptoms. Support from others — family, friends, employer, teachers — can help you cope with narcolepsy.

Migraine headaches are recurrent throbbing or pulsatile headaches often associated with a prodrome, nausea, vomiting, photophobia, and phonophobia. When they occur, the prodromes are characterized by visual scintillations, scotomas, dizziness, or tinnitus
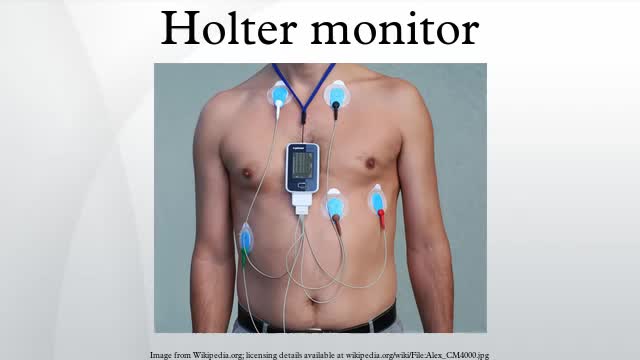
Holter monitoring, electrocardiogram or echocardiogram are only recommended if a cardiac cause (e.g., arrhythmias, possible cardiac syncope, myocardial ischemia) is suspected.

The "Get up and go" test is most commonly used to assess postural stability. In this test, the physician instructs the patient to stand up from a chair without assistance, walk a short distance, turn around, return, and sit down again. If the patient is unsteady or has difficulties during the test, further evaluation is necessary.
Vertebrobasilar insufficiency is typically secondary to emboli, thrombi, or arterial dissection. The labyrinth and brainstem are commonly affected, and symptoms may include vertigo, dizziness, dysarthria, diplopia, and numbness.
