- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
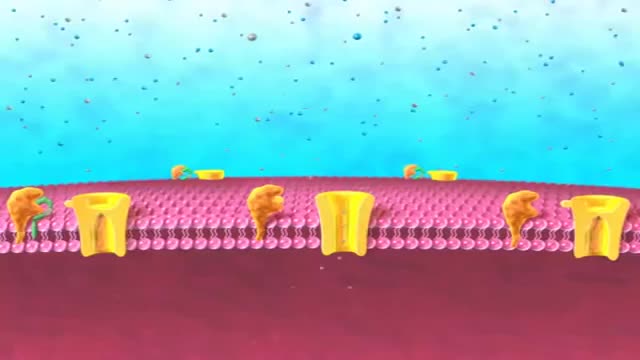
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
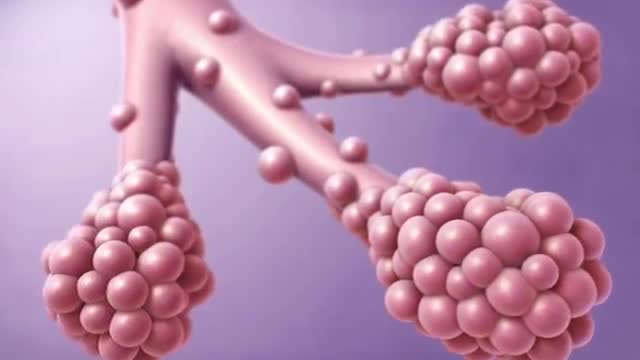
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
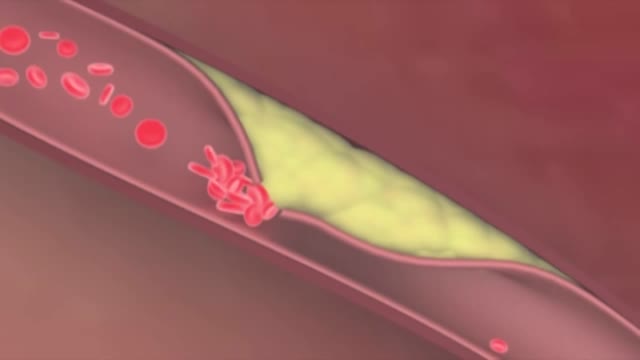
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Latest videos

Foot drop is a gait abnormality in which the dropping of the forefoot happens due to weakness, irritation or damage to the common fibular nerve including the sciatic nerve, or paralysis of the muscles in the anterior portion of the lower leg. It is usually a symptom of a greater problem, not a disease in itself.
Honeymoon palsy from another individual sleeping on and compressing one's arm overnight. Saturday night palsy from falling asleep with one's arm hanging over the arm rest of a chair, compressing the radial nerve
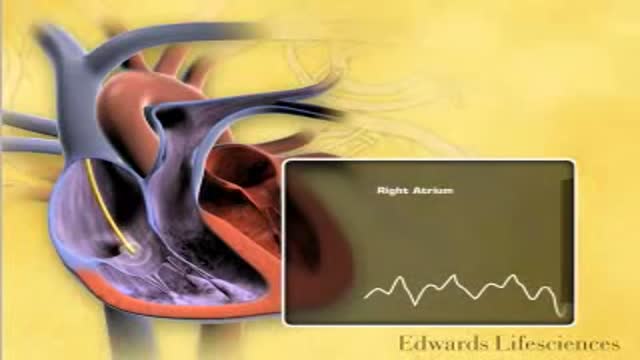
Pulmonary capillary wedge pressure (PCWP) provides an indirect estimate of left atrial pressure (LAP). Although left ventricular pressure can be directly measured by placing a catheter within the left ventricle, it is not feasible to advance this catheter back into the left atrium. LAP can be measured by placing a special catheter into the right atrium then punching through the interatrial septum; however, for obvious reasons, this is not usually performed because of damage to the septum and potential harm to the patient.

Pulmonary edema is almost always treated in the emergency room or hospital. You may need to be in an intensive care unit (ICU). Oxygen is given through a face mask or tiny plastic tubes are placed in the nose. A breathing tube may be placed into the windpipe (trachea) so you can be connected to a breathing machine (ventilator) if you cannot breathe well on your own. The cause of edema should be identified and treated quickly. For example, if a heart attack has caused the condition, it must be treated right away. Medicines that may be used include: Diuretics that remove excess fluid from the body Medicines that strengthen the heart muscle, control the heartbeat, or relieve pressure on the heart
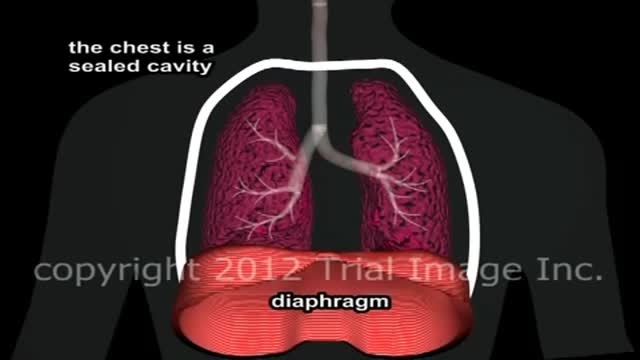
Pulmonary edema Email this page to a friend Email this page to a friend Facebook Twitter Google+ Pulmonary edema is an abnormal buildup of fluid in the lungs. This buildup of fluid leads to shortness of breath. Causes Pulmonary edema is often caused by congestive heart failure. When the heart is not able to pump efficiently, blood can back up into the veins that take blood through the lungs. As the pressure in these blood vessels increases, fluid is pushed into the air spaces (alveoli) in the lungs. This fluid reduces normal oxygen movement through the lungs. These two factors combine to cause shortness of breath.
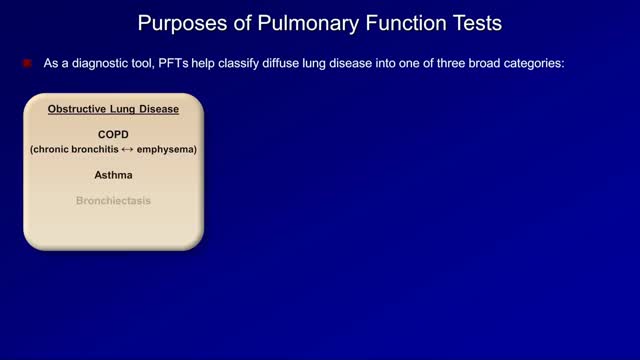
Pulmonary function tests are a broad range of tests that measure how well the lungs take in and exhale air and how efficiently they transfer oxygen into the blood. Spirometry measures how well the lungs exhale.
Idiopathic pulmonary fibrosis (IPF) is defined as a specific form of chronic, progressive fibrosing interstitial pneumonia of unknown cause, primarily occurring in older adults, limited to the lungs, and associated with the histopathologic and/or radiologic pattern of usual interstitial pneumonia (UIP).[1] Signs and symptoms The clinical symptoms of idiopathic pulmonary fibrosis are nonspecific and can be shared with many pulmonary and cardiac diseases. Most patients present with a gradual onset (often >6 mo) of exertional dyspnea and/or a nonproductive cough. Approximately 5% of patients have no presenting symptoms when idiopathic pulmonary fibrosis is serendipitously diagnosed.
Obstructive lung disease is a category of respiratory disease characterized by airway obstruction. Many obstructive diseases of the lung result from narrowing of the smaller bronchi and larger bronchioles, often because of excessive contraction of the smooth muscle itself. It is generally characterized by inflamed and easily collapsible airways, obstruction to airflow, problems exhaling and frequent medical clinic visits and hospitalizations. Types of obstructive lung disease include; asthma, bronchiectasis, bronchitis and chronic obstructive pulmonary disease (COPD). Although COPD shares similar characteristics with all other obstructive lung diseases, such as the signs of coughing and wheezing, they are distinct conditions in terms of disease onset, frequency of symptoms and reversibility of airway obstruction.[1] Cystic fibrosis is also sometimes included in obstructive pulmonary disease

Tuberculosis (TB) is a disease caused by bacteria called Mycobacterium tuberculosis. The bacteria usually attack the lungs, but they can also damage other parts of the body. TB spreads through the air when a person with TB of the lungs or throat coughs, sneezes, or talks. If you have been exposed, you should go to your doctor for tests. You are more likely to get TB if you have a weak immune system. Symptoms of TB in the lungs may include A bad cough that lasts 3 weeks or longer Weight loss Loss of appetite Coughing up blood or mucus Weakness or fatigue Fever Night sweats

The Most Important Heart Tests for Those Being Evaluated for Heart Disease To be sure, there are a number of good cardiac screening tests that should be included in any comprehensive preventive and diagnostic cardiac assessment. From all the options available in the massive cardiologist toolbox to assess basic heart function, these are the tests I recommend: Electrocardiogram (EKG) Echocardiogram Exercise/Nuclear Stress Test Holter Monitoring BNP Test
Use lifestyle changes Quit smokingQuit smoking. Avoid secondhand smoke too. ... Exercise . There are lots of ways that exercise boosts your heart health. ... Eat a heart-healthy diet . The way you eat can help you control your cholesterol and blood pressure. Stay at a healthy weight .

An increased prevalence of cardiovascular disease (CVD) has been found in women of childbearing age,[1] with the presence of CVD in pregnant women posing a difficult clinical scenario in which the responsibility of the treating physician extends to the unborn fetus. Profound changes occur in the maternal circulation that have the potential to adversely affect maternal and fetal health, especially in the presence of underlying heart conditions. Up to 4% of pregnancies may have cardiovascular complications despite no known prior disease. The European Society of Cardiology has published guidelines on the management of cardiovascular disease during pregnancy.[

each type of heart problem requires different treatment but may share similar warning signs. It is important to see your doctor so that you can receive a correct diagnosis and prompt treatment. Learn to recognize the symptoms that may signal heart disease. Call your doctor if you begin to have new symptoms or if they become more frequent or severe. Symptoms of Coronary Artery Disease The most common symptom of coronary artery disease is angina, or chest pain. Angina can be described as a discomfort, heaviness, pressure, aching, burning, fullness, squeezing, or painful feeling in your chest. It can be mistaken for indigestion or heartburn. Angina may also be felt in the shoulders, arms, neck, throat, jaw, or back. Other symptoms of coronary artery disease include: Shortness of breath Palpitations (irregular heart beats, or a "flip-flop" feeling in your chest) A faster heartbeat Weakness or dizziness Nausea Sweating
Osteoporosis is a disease that weakens bones over time. Because of this, it puts you at risk for breaking a bone. Postmenopausal osteoporosis is the most common form of osteoporosis. It affects many women after menopause, leaving some women at high risk for fracture. - See more at: https://www.prolia.com/postmenopausal-osteoporosis/deeper-look/?WT.z_co=A&WT.z_in=PMO&WT.z_ch=PDS&WT.z_st=Site1&WT.z_mt=Broad&WT.z_pdskw=www%20osteoporosis&WT.z_ag=Osteoporosis%20Information%20-%20Broad&WT.z_se=G&WT.srch=1&WT.z_prm=DSE__&WT.mc_id=A_PMO_PDS_G_DSE___Broad_www%20osteoporosis_Osteoporosis%20Information%20-%20Broad#sthash.x5Ys3Now.dpuf

Avoid Osteoporosis, Build Bone Density With Upper Body Exercises

How to prepare for your bone density scan
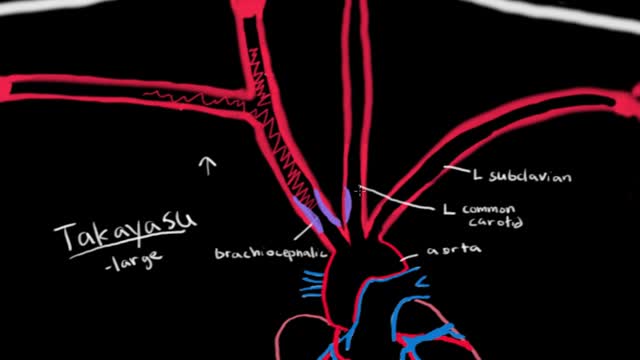
Takayasu's arteritis (tah-kah-YAH-sooz ahr-tuh-RIE-tis) is a rare type of vasculitis, a group of disorders that cause blood vessel inflammation. In Takayasu's arteritis, the inflammation damages the aorta — the large artery that carries blood from your heart to the rest of your body — and its main branches. The disease can lead to blockages or narrowed arteries (stenosis) or abnormally dilated arteries (aneurysms). Takayasu's arteritis can also lead to arm or chest pain and high blood pressure and eventually to heart failure or stroke. If you don't have symptoms, you may not need treatment. Or you may need medications to control the inflammation in the arteries and prevent complications. But even with treatment, relapses are common.

Giant cell arteritis is an inflammation of the lining of arteries. Most often, it affects the arteries in your head, especially those in your temples. For this reason, giant cell arteritis is sometimes called temporal arteritis. Giant cell arteritis frequently causes headaches, scalp tenderness, jaw pain and vision problems. If left untreated, it can lead to stroke or blindness. Prompt treatment with corticosteroid medications usually relieves symptoms of giant cell arteritis and may prevent loss of vision. You'll likely begin to feel better within days of starting treatment. But even with treatment, relapses are common. You'll need to visit your doctor regularly for checkups and treatment of any side effects from taking corticosteroids.

Giant cell arteritis is an inflammation of the lining of your arteries. Most often, it affects the arteries in your head, especially those in your temples. For this reason, giant cell arteritis is sometimes called temporal arteritis. Giant cell arteritis frequently causes headaches, scalp tenderness, jaw pain and vision problems. If left untreated, it can lead to stroke or blindness. Prompt treatment with corticosteroid medications usually relieves symptoms of giant cell arteritis and may prevent loss of vision. You'll likely begin to feel better within days of starting treatment. But even with treatment, relapses are common. You'll need to visit your doctor regularly for checkups and treatment of any side effects from taking corticosteroids.

Polyarteritis nodosa Email this page to a friend Email this page to a friend Facebook Twitter Google+ Polyarteritis nodosa is a serious blood vessel disease. The small and medium-sized arteries become swollen and damaged. Causes Arteries are the blood vessels that carry oxygen-rich blood to organs and tissues. The cause of polyarteritis nodosa is unknown. The condition occurs when certain immune cells attack the affected arteries. More adults than children get this disease. The tissues that are fed by the affected arteries do not get the oxygen and nourishment they need. Damage occurs as a result. People with active hepatitis B or hepatitis C may develop this disease.
