- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Latest videos

Abnormal Eye Lid Positions Ptosis
Alicia Berger
6,565 Views • 3 years ago
Abnormal Eye Lid Positions Ptosis

Gastric Lavage Video
Alicia Berger
15,679 Views • 3 years ago
Gastric Lavage Video
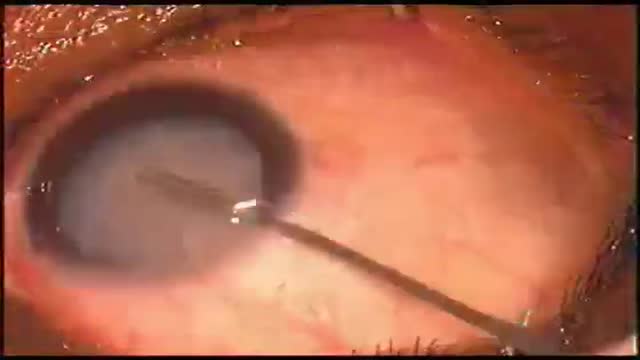
Eye Phacoemulsification
Alicia Berger
6,283 Views • 3 years ago
Eye Phacoemulsification

Pterygium Excision with Auto Conjunctival Graft
Alicia Berger
8,563 Views • 3 years ago
Pterygium Excision with Auto Conjunctival Graft

Ocular Movement Examination
Alicia Berger
7,062 Views • 3 years ago
Ocular Movement Examination

Keratectomy with Amniotic Membrane Graft Eye
Alicia Berger
7,142 Views • 3 years ago
Keratectomy with Amniotic Membrane Graft Eye

Eye Lid Tarsal Fracture Surgery
Alicia Berger
7,348 Views • 3 years ago
Eye Lid Tarsal Fracture Surgery

Eye Lid Partial Tarsectomy Surgery
Alicia Berger
6,112 Views • 3 years ago
Eye Lid Partial Tarsectomy Surgery

Eye Lid Jones Procedure
Alicia Berger
5,999 Views • 3 years ago
Eye Lid Jones Procedure

Arteriolotomy Open Heart Surgery
Alicia Berger
10,874 Views • 3 years ago
Arteriolotomy Open Heart Surgery

Pulmonary Artery Swan Ganz Catheter
Alicia Berger
9,508 Views • 3 years ago
Pulmonary Artery Swan Ganz Catheter

Hemodialysis Machine Setup
Alicia Berger
8,548 Views • 3 years ago
Hemodialysis Machine Setup

Diabetic Nephropathy Animation 3D
Alicia Berger
12,211 Views • 3 years ago
Diabetic Nephropathy Animation 3D

Ligation of Aneurysm in ArterioVenous Malformation
Alicia Berger
7,247 Views • 3 years ago
Ligation of Aneurysm in ArterioVenous Malformation

Acute Renal Failure for Nursing
Alicia Berger
11,295 Views • 3 years ago
Acute Renal Failure for Nursing
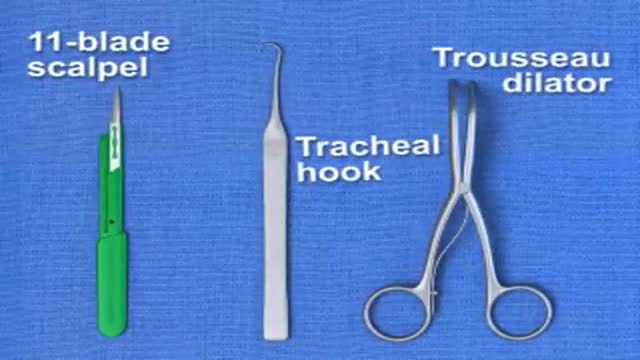
Traditional Surgical Cricothyrotomy
Alicia Berger
9,909 Views • 3 years ago
Traditional Surgical Cricothyrotomy

Cricothyrotomy Quick Airway Access
Alicia Berger
8,702 Views • 3 years ago
Cricothyrotomy Quick Airway Access

Mechanism of Type 2 Diabetes Animation
Alicia Berger
10,413 Views • 3 years ago
Mechanism of Type 2 Diabetes Animation

Peritoneal Dialysis for Kidney Disease
Alicia Berger
14,419 Views • 3 years ago
Peritoneal Dialysis for Kidney Disease

Hemodialysis Introduction for Kidney
Alicia Berger
10,690 Views • 3 years ago
Hemodialysis Introduction for Kidney
Showing 264 out of 265
