- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Latest videos

Changing Dressing Wounds
Harvard_Student
7,196 Views • 2 years ago
Changing Dressing Wounds

Thoracocentesis Removing 1200CC Pleural Fluid
Harvard_Student
9,026 Views • 2 years ago
Thoracocentesis Removing 1200CC Pleural Fluid

Bandages Different Applications
Harvard_Student
6,915 Views • 2 years ago
Bandages Different Applications
Drawing up from a vial
Harvard_Student
6,953 Views • 2 years ago
Drawing up from a vial

Feeding Tube
Harvard_Student
6,095 Views • 2 years ago
Feeding Tube
Burns Handling Thermal Electrical Chemical
Harvard_Student
7,006 Views • 2 years ago
Burns Handling Thermal Electrical Chemical
Drawing from an Ampoule
Harvard_Student
7,616 Views • 2 years ago
Drawing from an Ampoule
Insulin Pen
Harvard_Student
6,653 Views • 2 years ago
Insulin Pen

Intramuscular Injection Technique
Harvard_Student
11,828 Views • 2 years ago
Intramuscular Injection Technique

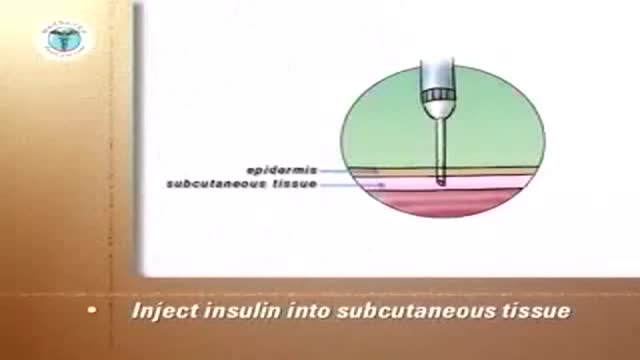
Injecting Insulin Techniques
Harvard_Student
8,863 Views • 2 years ago
Injecting Insulin Techniques

Basic CardioVascular Clinical Exam
Harvard_Student
8,255 Views • 2 years ago
Basic CardioVascular Clinical Exam

Percussion Technique
Harvard_Student
7,784 Views • 2 years ago
Percussion Technique
Peripheral Venous Access Technique Video
Harvard_Student
9,336 Views • 2 years ago
Peripheral Venous Access Technique Video
Male Foley Catheterization Technique
Harvard_Student
10,384 Views • 2 years ago
Male Foley Catheterization Technique
Arterial Blood Gas Sampling Technique Video
Harvard_Student
8,266 Views • 2 years ago
Arterial Blood Gas Sampling Technique Video
Phlebotomy Drawing Blood from Veins
Harvard_Student
10,927 Views • 2 years ago
Phlebotomy Drawing Blood from Veins

Basic Abdominal Clinical Exam
Harvard_Student
8,143 Views • 2 years ago
Basic Abdominal Clinical Exam

Thyroid Gland Clinical Exam Video
Harvard_Student
8,807 Views • 2 years ago
Thyroid Gland Clinical Exam Video

Female Foley Catheterization Technique
Harvard_Student
10,824 Views • 2 years ago
Female Foley Catheterization Technique

Chest Expansion Clinical Exam
Harvard_Student
18,092 Views • 2 years ago
Chest Expansion Clinical Exam
Showing 273 out of 274
