Últimos vídeos
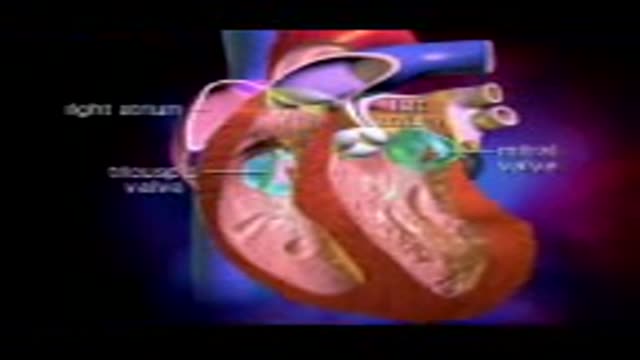
Heart Valves

Gastrointestinal GI Drug Delivery

Imperforate Hymen

Lower Face Lift Awake Plastic Surgery

Pelvic lymphadenectomy
Dissection and Cannulation of Cadaveric Kidney

Traumatic Urinary Bladder Groin Injury

New Phacoemulsification Horizontal Chopping

Eye Surgery penetrating Keratoplasty

Eye Cyst Removal By Vitrectomy

Eye Surgery Trabeculectomy

Eye Surgery C Lasik

Abnormal Eye Lid Positions Ptosis

Gastric Lavage Video
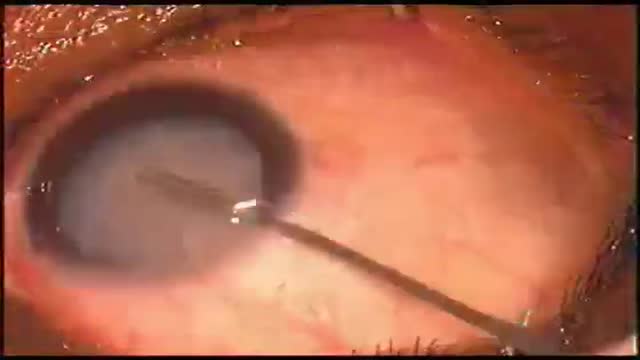
Eye Phacoemulsification

Pterygium Excision with Auto Conjunctival Graft

Ocular Movement Examination

Keratectomy with Amniotic Membrane Graft Eye

Eye Lid Tarsal Fracture Surgery

Eye Lid Partial Tarsectomy Surgery
Showing 275 out of 276
