- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Latest videos

This minimally invasive procedure cures acid reflux without resorting to a large abdominal incision. It also decreases recovery time. ~ Detroit Medical Center
A patient suffering from Trigeminal Neuralgia (extreme facial pain) has breakthrough neurosurgery, microvascular decompression, to resolve the pain & restore quality of life.~ Detroit Medical Center

DMC Pediatric Heart Specialist Doctor Peter Karpawich is the first in the state to use minimally invasive surgery to repair a damaged pacemaker on a pediatric patient, helping her lead a more active, fulfilling lifestyle. ~ Detroit Medical Center

Clogged leg arteries can be opened through a minimally invasive procedure with the SILVERHAWK, a mini drill with a tiny rotating blade for cutting away plaque. The procedure only involves a tiny puncture in the patient's groin. ~ Detroit Medical Center

Its technical name is selective laser trabeculoplasty or SLT. It's a virtually painless, minimally invasive procedure that provides several benefits over conventional treatments for glaucoma. ~ Detroit Medical Center

Lasik eye surgery at the Detroit Medical Center's Advanced Laser and Clear Vision Center offer patients pain-free, life-changing procedures that correct nearsightedness, farsightedness, and astigmatism. ~ Detroit Medical Center
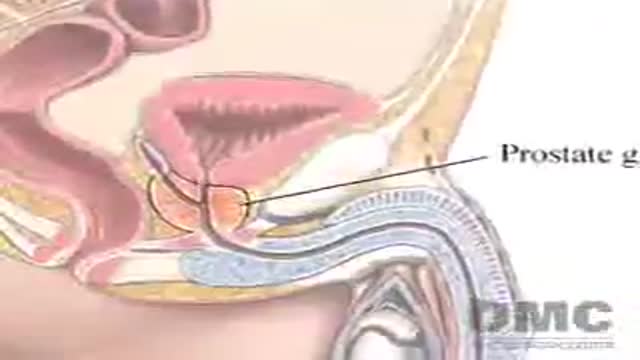
Doctors at Detroit Medical Center are treating prostate cancer with cryoablation, an innovative procedure that freezes cancer cells and preserves surrounding tissue. Patients usually return home the same day as the treatment. ~ Detroit Medical Center
This minimally invasive procedure connects electrodes to the brain and places a pacemaker-like device under the skin. When activated, electrical impulses minimize shaking due to "dyskinesia syndrome" in patients with Parkinson's disease. ~ Detroit Medical Center

As one of the first pediatric centers in the United States to use a new state-of-the-art MRI machine designed especially for kids, Children's Hospital of Michigan continues to deliver world-class, patient-friendly health care. ~ Detroit Medical Center

This revolutionary new procedure is generally recommended for patients with hip arthritis who are less than 60 years old. ~ Detroit Medical Center

Doctors at the Detroit Medical Center pioneer laparoscopy procedures and other minimally invasive techniques that result in less pain, fewer risks, and quicker recovery time for surgical patients. ~ Detroit Medical Center

"Targeted" radiation therapy goes right to the problem, not throughout your system. Moreover, discomfort is minimal. ~ Detroit Medical Center

Re-educating the legs to walk again is the ultimate goal of this therapy for those who have suffered a stroke. ~ Detroit Medical Center

About 15 minutes of vibration produces similar results to an hour of conventional resistance therapy, and produces less stress on joints, ligaments and tendons. ~ Detroit Medical Center

This high technology apparatus for the forearm is helping to restore hand movement in stroke patients. ~ Detroit Medical Center

Less pain and no incisions are just two benefits of robotically assisted surgery thanks to the da Vinci Surgical System. ~ Detroit Medical Center

Urethroplasty is a surgical procedure to correct scar tissue blockage of the urethra called urethral stricture. ~ Detroit Medical Center

At Hutzel Women's Hospital, Dr. Giancarlo Mari performs breakthrough in-utero surgery to save the lives of high-risk twins developing with a rare "shared" circulatory problem. ~ Detroit Medical Center
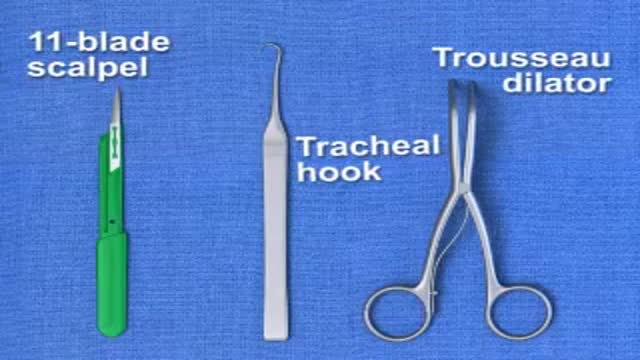
Brief animation demonstrating emergency surgical cricothyrotomy; created with Lightwave 9.3
This involves inserting a tube through the nasal passage, into the stomach
