Latest videos

The essential steps of a translaminaterminalis approach for removal of craniopharyngiomas
Access to processes within the skull base with lateral extension to the pterygopalatine fossa are reached by combined subfrontal osteotomy and Le Fort I osteotomy
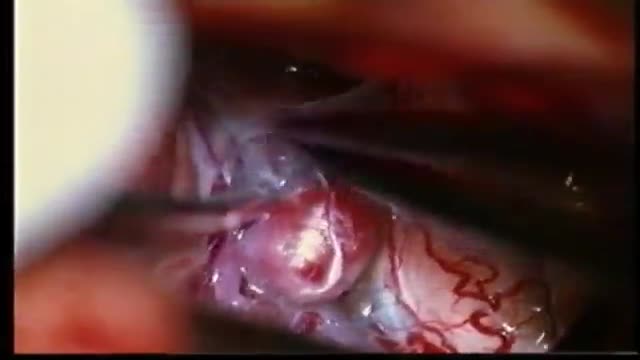
trigeminal neuralgia can be caused by a vessel loop nearby the entry zone of the trigeminal nerve at the brainstem. a vessel loop is mobilized and transposed and secured with a teflon paddy. the paddy is fixed with tissucol , a fibrin glue without evident neurotoxicity. the long term result of the jannetta procedure regarding pain control is excellent
Acoustic Neuroma
Extradural approach via Orbito-Zygomatic Craniotomy
Resection of a glioblastoma multiforme, a very malignant, aggressive brain tumor.

Thoracoscopic Discectomy
ANEURYSMS OF THE CEREBRAL VESSELS CAUSE SUBARACHNOID HEMORRHAGE. MICRONEUROSURGICAL CLIPPING ELIMINATES DEFINITIVE THE RISK OF RERUPTURE, ENABLES TO TREAT VASOSPASMS AND ELIMINATES THE NEED FOR RE-ANGIOGRAPHIES. INTRAOPERATIVE PUNCTURE CHECKS IMMEDIATLY THE ELIMINATION OF THE ANEURYSM.

An older patient with stomach pain, and the typical heart burning. We did some biopsies for evaluation of dyplasia.

Endoscopic third ventriculostomy in a patient with obstructive hydrocephalus

lesions at the anterior skull base invading the paranasal area and the paracavernous area can be reached without brain retraction by the shown subfrontal approach. it enables to control the paranasal sinus, optic nerve, periorbital tissue, carotid artery and pituary gland. reconstruction is not easy... but cosmetically appealing. CSF leaks are rare with the use of fascia lata and tissucol ( fibrin glue). osseous reconstruction is done by microsrews and calciumpyrophosphate ( norian, synthes).

A quick look at an early stage stomach abnormality.

En Bloc Esophageal Mucosectomy, an experimental technique for the endolumenal management of Barrett's related dysplasia and neoplasia. High grade dysplasia is in indication for esophagectomy; however esophagectomy has a mortality rate up to 12 percent, and up to 56 percent of patients may develop s...erious post-operative complications. Multiple ablated lesions can progress under the neo-squamous layer, leading to buried Barrett's mucosa. With conventional piecemeal EMR, cautery effect limits evaluation in areas of interest, Barrett's epithelium is left behind, tissue is not evaluated in situ and invasive lesions may be missed due to incomplete sampling. A new technique, en bloc esophageal mucosectomy, or EEM, was developed. The technique begins with conventional EMR in the proximal esophagus to access the submucosal space. Conventional EMR is being performed here. The mucosa is resected using an electrothermal snare. The mucosal defect from the first EMR is seen here. EMR is then repeated on the opposing wall. Sequential EMR creates a complete concentric mucosal defect. In the following sequence the completely detached column of mucosa can be seen, bounded by submucosa and muscularis propria layers. Here in the stomach, the endoscope is retroflexed and is covered by a sleeve of esophageal mucosa which has been freed to the GE junction and inverted. This sequence demonstrates a double snare technique. This snare is alongside the endoscope. The snare has been passed through the working channel. The working channel snare is pulled back, and the snare alongside the scope is used to grasp the mucosal column. With tension on the column the working channel snare can be threatened and advanced. This sequence shows the snare as it is being passed down to the GE junction. At the GE junction, the snare is tightened and cautery is applied. This frees the column of mucosal tissue from the remaining attachment. The endoscope is then withdrawn. Then detached mucosal column can be grasped with a snare and retrieved. In the following sequence, the long column of mucosa is being withdrawn via the overtube. Here, endoscopic forceps have been passed through the column to demonstrates the concentric nature of the specimen. The length of mucosa can be seen here alongside 2 conventional EMR specimens. Approximately 15cm of tissues was removed in this case. On endoscopy immediately following the resection, there is no bleeding or evidence of perforation in the area of resection. The endoscope is advanced and the exposed submucosa can be appreciated down to the GE junction. This is the low power view of the histologic specimen generated by EEM. Metaplastic tissue adjacent to a dysplastic focus would be completely removed. With a high power view, the layers of the esophagus can be appreciated. The epithelium, lamina propria, muscularis mucosa and submucosa are visible, with no cautery artifact in the area of interest. The technique would remove metplasia, low grade dysplasia, high grade dysplasia, and intramucosal carcinoma, as well a T 1 a lesions. All the animals in this series tolerated the procedure well. A total of five non-survival procedures and 4 survival procedures were performed. In the survival procedures, all four swine thrived in the post-operative period. Two swine were then survived for 9 days following the procedure. On post —op day nine, after passing into the upper esophagus, the proximal margin of the mucosectomy is seen here. Healing appears to be occurring. There is no evidence of leak, and no stricting is seen at 9 days down to the GE junction Passing into the stomach, some residual feed can be seen. Two swine were then survived for 13 days. On this follow-up endoscopy, the area of the mucosectomy is again healing. There was a loose stricture in both animals and both were easily traversed with a 9.8 mm gastroscope. There was a gross appearance of re-epitheliazation in some areas. It is notable that the stricture was present in the proximal esophagus with no narrowing distally. At necropsy there was not eviden

This video clip shows an upper track endoscopy of A 75 year-old female, presented with severe adominal pain since three days. Endoscopy displays a deep ulcer at the lesser curvature of the stomach. This patient has a klatskin´s tumor (bile duct bifurcation).
Purpose The complication rate in patients treated with the Linton procedure was unacceptably high. SEPS is minimal invasive treatment modality for chronic venous insufficiency and venous ulcers. Materials and Methods252 limbs of 229 patients who underwent SEPS procedure and/or safenous vein ablati...on from May 2003 to January 2008. Tourniquet was not used and two-port technique was preferred for operation. Skin graft was not used. Honeysoft (medical honey) was used for wound care in selected cases. Results According to CEAP clinical Classification 112 limbs were class 6, 70 limbs (class 5), 70 limbs (Class4) respectively. Greater saphenous vein stripping and/or high ligation, and varicose vein excision accompanied SEPS in 241limbs who had combined Sapheno-femoral junction and perforator vein insufficiencyand SEPS was performed alone 23 limbs who had recanalised deep venous thrombosis (19) and PVI alone(4). Mean patient follow-up was 35 months. No early deaths or thromboembolism occurred. Complications included severe subcutaneous emphysema(1), neuralgia (7), 1 year later cellulites (1). Ulcers healed in 124 limbs in two months and 58 limbs in 3 months. ulcer recurrence was seen on 12(%6.6) limbs. Clinical severity and disability scores improved significantly after surgery. Conclusion All venous ulcers healed with SEPS combined or not ablation of superficial venous reflux and remain healed 5 year period and symptom-free except recurrent ulcers during the long-term follow-up. SEPS is an effective and safety treatment modality.

Cholecystectomy

Surgical technique: A 3cm skin incision under spinal or general anesthesia, depending on the patients’ preference, starts half way the line between the superior anterior iliac spine towards the midline in a 30° angle to the pubic tubercle. Scarpa’s fascia is opened as well as the external obliq...ue aponeurosis. By using this skin line incision the internal ring will be immediately visualized. Although it is important to look for both direct and indirect hernias evaluating the groin, we do not taper the cord and directly evaluate the ring for indirect hernias. In case of an indirect hernia the sac is reduced or resected according to the preference of the surgeon and the preperitoneal space is entered bluntly through the dilated internal ring. In case of a direct hernia the approach slightly differs. One could prefer to open the transversalis fascia through the internal ring over a few centimeters or you can open the fascia more medially, at the site of the direct hernia. As primary point of concern the epigastric vessels should be identified and retracted softly upwards. Then a gauze can be introduced into the preperitoneal space and by doing so most of the space needed medially will be created. Then one can already palpate Cooper’s ligament and the pubic bone. Laterally to the internal ring more digital dissection is needed to create just the appropriate space for the mesh. By placing the mesh it is important not to introduce the mesh too medially. Laterally of the internal ring an adequate overlap of the mesh is necessary, especially in indirect hernias. No splitting of the mesh seems necessary. The patient will be asked to strain and push on the ring to control its place and to check adequate spreading of the mesh to cover the whole myopectineum of Fruchaud. One single stitch of vicryl 3/0 is placed taking both the fascia transversalis and the mesh.

Laparoscopic Appendicectomy

Truncal Vagotomy and Pyloroplasty

Appendectomy with corpus Luteal rupture
