- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Latest videos

This video demonstrates the use of an episiotomy to facilitate vaginal delivery of a baby
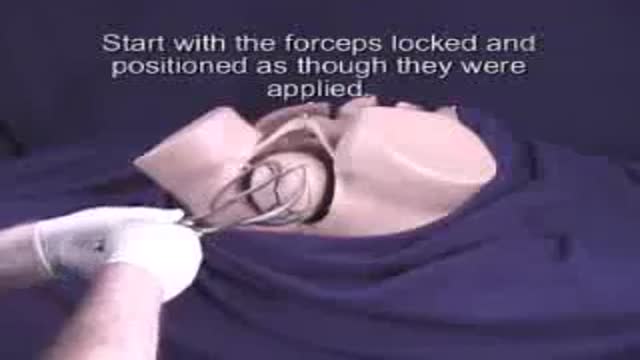
Forceps are used to assist in labor and delivery. Forceps delivery is considered an operative obstetric procedure

The umbilical cord is wrapped around the baby's neck in about 25% of deliveries. If loose, it usually has no impact on the delivery. If tight, it may need to be relieved before delivery of the baby can proceed safely

The bulb syringe is readily available, safe tool for clearing the airway of a newborn infant
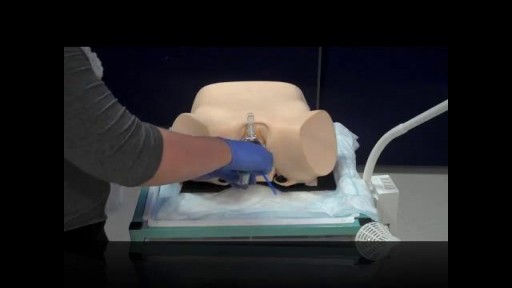
Pelvic examinations during labor are used for several purposes, among them assessment of cervical dilatation, effacement, station of the presenting part, presentation, position, and pelvic capacity.Instruction in these techniques is particularly important for those health care providers involved in labor management, including physicians, nurses, midwives, paramedics and EMT personnel.
demonstrates the use of an oropharyngeal device to maintain the patient's airway

how to obtain intravenous access through cutting down over a large peripheral vein

basic subcutaneous (SQ) injection techniques

the technique of insertion of a tube into the abdomen to diagnose intra-abdominal bleeding

the technique of insertion of a tube into the pericardial sac to remove fluid or blood, improving cardiac function
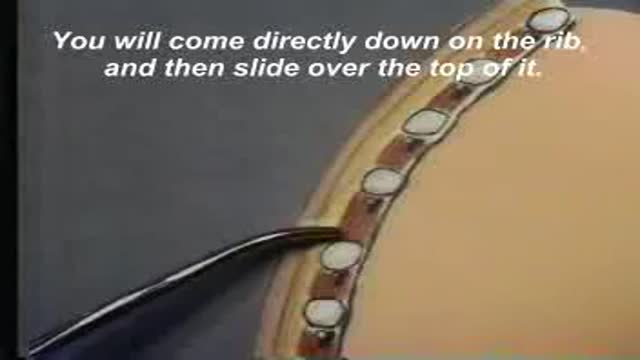
A video showing the insertion of chest tube
a video showing how to suture a wound
Eye Treatment

Catheterization of the Male and Female

It demonstrates basic suturing techniques as might be applied in an emergency room setting.
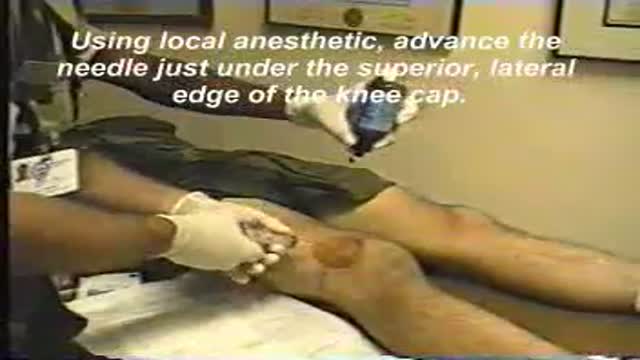
Using models and actual patient video, the aspiration of a traumatically injured knee joint is demonstrated.

This video demonstrates pelvic adhesions found in a patient with endometriosis during laparoscopic surgery.

This video shows a chocolate cyst of the ovary during laparoscopy. These common ovarian cysts are often found with endometriosis or other hemorrhagic conditions within the ovary

This video demonstrates how to treat venereal warts or condyloma using a cryosurgery technique.

This video shows an ovarian cyst and its removal using a laparoscopic technique.
