- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Latest videos

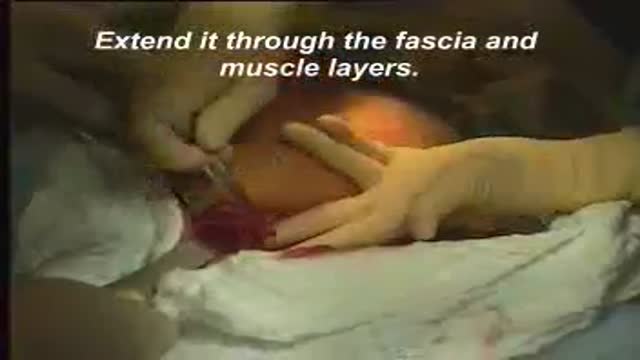
Laparotomy : opening the abdomen

Total abdominal hysterectomy

A video showing how to suture the uterus during ceseran section
A video showing the repair of episiotomy
A video showing the steps of cesarean section surgery

Delivery of the placenta
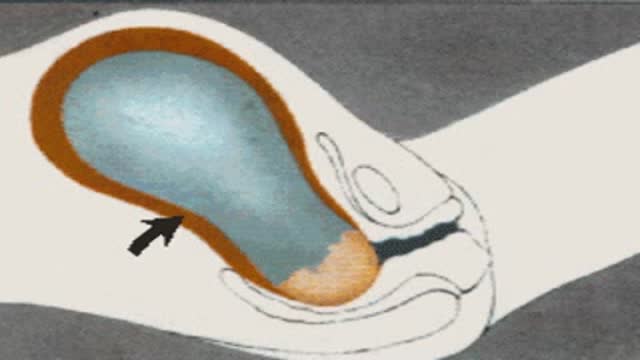
A video showing vaginal delivery

Continuous Lumbar Epidural

Leopold's Maneuvers Video

A video showing amniotomy

An U/S showing first trimesteric scan

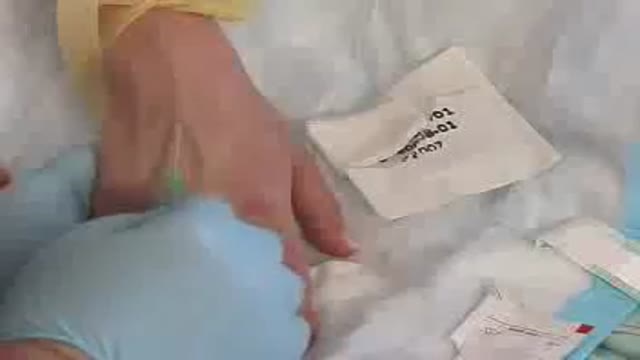
How to obtain a blood sample

Inserting a nasogastric tube
Starting an IV

Foley Catheter Insertion
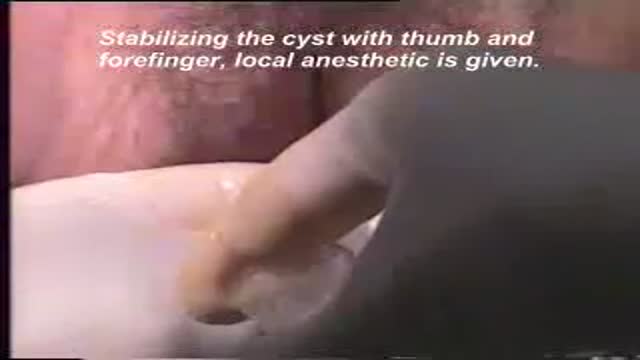
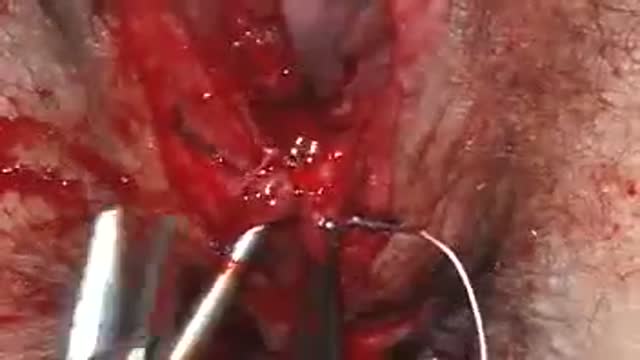
A video showing drainage of a bartholin cyst

A video showing how to insert the Intra Uterine Device (IUD)

How to remove the Intra Uterine Device (IUD)
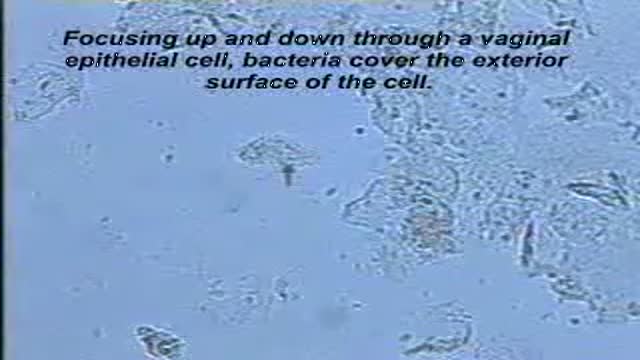
A clue cell appears smudged, with indistinct contents and fuzzy, poorly defined borders.

A normal vaginal epithelial cell is clear, with recognizable contents, and sharp, distinct cell borders.
