Latest videos

UPDATE 2/6/15: A new version of this animation is now available! https://www.youtube.com/watch?v=E1ljClS0DhM
This 3D medical animation depicts the surgical removal of the appendix (appendectomy) using laparoscopic instruments. The surgery animation begins by showing an inflamed appendix (appendicitis), followed by the placement of the laparoscope. Afterward, one can see the surgical device staple, cut and remove the inflamed appendix. Following the removal of the appendix the abdomen is flushed with a sterile saline solution to ensure all traces of infection have been removed.
ANCE00183

"Laparoscopic Placement of a
Peritoneal Dialysis Catheter"
Houston Methodist DeBakey Heart & Vascular Center, presents a cardiovascular procedure featuring Eric K. Peden, MD, Shri Timbalia, MD, and Kenneth Livingston as they demonstrate “Laparoscopic Placement of a
Peritoneal Dialysis Catheter".
Surgery: Eric K. Peden, MD, Shri Timbalia, MD, and Kenneth Livingston
Narration: Kenneth Livingston
** This medical education program may contain graphic content. **
_________________________________
A DeBakey CV Education event
Presented by Houston Methodist DeBakey Heart & Vascular Center.
Building on Dr. Michael E. DeBakey’s commitment to excellence in education, Houston Methodist DeBakey CV Education is an epicenter for cardiovascular academic and clinical educational programs that support the provision of optimal care to patients suffering from cardiovascular conditions and diseases.
FOR MORE INFORMATION
DeBakey CV Education:
https://www.houstonmethodist.o....rg/education/medical
For the latest education and training opportunities from DeBakey CV Education: http://bit.ly/HMdebakeyemail
Follow Us:
Facebook: https://www.facebook.com/debakeycvedu
Twitter: https://twitter.com/DeBakeyCVedu
Livestream: https://livestream.com/debakey
SmugMug: https://debakey.smugmug.com/
Want concise, relevant reviews of the hottest topics in CV medicine? Subscribe for FREE to the Methodist DeBakey Cardiovascular Journal for quarterly, peer-reviewed issues delivered to your door.
https://journal.houstonmethodist.org/

This surgical animation is for patient education and describes a laparoscopic colectomy, which is a type of minimally invasive surgery for colon cancer. Laparoscopic colectomy, also called minimally invasive colectomy, involves several small incisions in your abdomen. Instead of a big incision, the surgeon makes a few small cuts (0.5-1 centimeters) in the abdominal cavity to insert a surgical camera and instruments and perform the operation. A slightly bigger incision, about 3.5 centimeters wide, is made to remove the tumor.
When compared to traditional open surgery, laparoscopic colectomy can result in much less pain and swifter recovery. Depending on the procedure, most laparoscopic colectomy patients leave the hospital and return to normal activities more quickly than patients recovering from open surgery.
Colorectal cancer is the second leading cause of cancer death in the United States.
For more information about 3d animation videos, please visit https://www.amerra.com
This medical animation shows laparoscopically assisted gallbladder removal surgery, or cholecystectomy. The animation begins by showing the normal anatomy of the liver and gallbladder. Over time, gallstones form within the gallbladder, blocking the cystic duct, and causing the gallbladder to become enlarged and inflamed. The procedure, sometimes called a "lap-chole", begins with the insertion of four trocar devices, which allow the physician to see inside the abdomen without making a large incision. Air is added to the abdominal cavity to make it easier to see the gall bladder. Next, we see a view through the laparascope, showing two surgical instruments grasping the gallbladder while a third severs the cystic duct. After the gallbladder is removed, the camera pans around to show that the cystic artery and vein, have already been clipped to prevent bleeding.
Item #ANIM026
For more information about living liver donor program, please visit https://cle.clinic/31rgy9F
Unlike open surgery that requires a large incision to access the liver, the laparoscopic procedure is performed with surgical tools and a camera inserted through a few half-inch holes in the abdomen of the living donor. Once the piece of the liver is dissected, the surgeon retrieves the graft through a small incision below the navel.
Liver transplant surgeon C.H David Kwon, MD, discusses the laparoscopic liver donor procedure more.
To learn more about Dr. Kwon, please visit https://cle.clinic/3Lvk9cv
If you liked the video hit like and subscribe for more!
#clevelandclinic #livingdonor #livertransplantation #livertransplant #organdonation #laparoscopicsurgeon #laparoscopysurgery

http://www.nucleushealth.com/ - This 3D medical animation shows the cause and laparoscopic treatment of a ventral incisional hernia. If you have had abdominal surgery in the past, a ventral incisional hernia may appear at the site of your surgical scar. Your intestine may push through a weakened spot in the tissue between your abdominal muscles creating a bulge beneath your skin. If your hernia is not repaired, complications may occur.
#VentralHernia #VentralIncisionalHernia #IncisionalHernia
ANH11053

Although it demands an advanced set of skills that remain substantially hard to do, many of the salient steps of “open” surgery, including suturing, are credibly “replicated” in its laparoscopic counterpart with the intention of achieving similar optimal results. This video demonstrates how to tie Laparoscopic Roeder's Knot. Laparoscopic Roeder's Knot is one of the oldest knots used in laparoscopic surgery. It is used most commonly during laparoscopic appendectomy surgery. Recent literature, though abundant with numerous reports pertaining to a variety of endoscopic knotting techniques and technologies, appears to lack scientific data but Roeder's knot is a time tasted extracorporeal slip knot that is secure for 6-8 mm diameter tubular structure.
For more information please contact:
World Laparoscopy Hospital
Cyber City, Gurugram, NCR DELHI
INDIA 122002
Phone & WhatsApp: +919811416838, + 91 9999677788

The video is about the evolution of the anatomic UCLA laparoscopic technique over 1325 cases and demonstrates the key steps of our operation to improve patient safety and outcomes.
Learn more at http://urology.ucla.edu

Dr. Neel Joshi, Clinical Chief, Department of Surgery at Cedars Sinai, describes his technique for trocar removal at the end of laparoscopic cholecystectomy.
#medicaleducation #laparoscopicsurgery

http://www.laparoscopyhospital.com
For the surgeon to develop the same level of proficiency and dexterity in the endoscopic environment as he may possess in open surgery is not a simple matter. The use of proper Mishra's Knot, are essential. Participating in an in-depth, systematic training program in a laboratory setting is essential before applying endoscopic Mishra's Knot techniques to humans. Successful acquisition of these Mishra's Knot skill requires that the surgeon be motivated to succeed and willing to invest the time and effort necessary to do so. Succumbing to the temptation of mechanical devices in lieu of acquiring the manual skills results in a questionable dependence on disposable technology and reduces the cost effectiveness of the minimally invasive approach. It is the adoption of Mishra's Knotting skills by the surgeon that will expand the surgeon's capability of performing increasingly advanced endoscopic surgical procedures.
For more information please contact:
World Laparoscopy Hospital
Cyber City, DLF Phase II, Gurgaon
NCR Delhi, 122002, India
Phone & WhatsApp: +919811416838, + 91 9999677788
contact@laparoscopyhospital.com

Laparoscopic surgery is now commonly used as a type of minimally invasive surgery, but what is it and why is it used?
Interested in learning more about minimally invasive techniques, or having surgery planned? Visit https://www.topdoctors.co.uk/doctor/charles-imber
✔ Follow us on Instagram: https://bit.ly/3fSrqXb
✔ Follow us on Facebook: https://bit.ly/3t5kGsW
✔ Follow us on Twitter: https://bit.ly/39TidKh

Visit our website to learn more about using Nucleus content for patient engagement and content marketing: http://www.nucleushealth.com/
#LaparoscopicColectomy #ColonSurgery #LargeIntestine
A colectomy is usually done to treat diseases that inflame your colon, a bowel obstruction, colon cancer, or a damaged or injured colon. The anatomy of the colon, and the laparoscopic procedure done to remove a portion of the colon, are depicted.
ANH18221
To license this video for patient education or content marketing, visit: http://www.nucleushealth.com/?utm_source=youtube&utm_medium=video-description&utm_campaign=tephernia-030615
An inguinal hernia is a bulging of the intestine through a defect or weak spot in the wall of the lower abdomen. This video shows how inguinal hernias form and how they are treated.
#TotalExtraperitonealLaparoscopicInguinalHerniaRepair #TEP #laparoscopy
ANCE00200

***************************************************************************
MEDICAL ANIMATION TRANSCRIPT:
Laparoscopic Ovarian Drilling (LOD)
A surgical treatment for women with PCOS
Women with PCOS usually have ovaries with a thick outer layer.
Ovarian drilling works by breaking through the thick outer surface and lowering the amount of testosterone made by the ovaries
A small incision is made in the abdomen.
Carbon dioxide gas is used to inflate the abdomen.
Very small holes are made in the ovaries.
Ovarian drilling can help restore ovulation and improve the chances of becoming pregnant.
***************************************************************************
*TimeStamps*
0:00 Introduction
0:15 Procedure of Laparoscopic Ovarian Drilling (LOD)
***************************************************************************
Let us watch this 3D video to understand what is Laparoscopic Ovarian Drilling for PCOS, why it is done, how well it works, and what to expect.
***************************************************************************
Get credible information on various health topics follow us on:
* Facebook: https://www.facebook.com/eremedium
* Instagram: https://www.instagram.com/eremedium/
* LinkedIn: https://www.linkedin.com/company/13197441/
* Twitter: https://twitter.com/eremedium
***************************************************************************
Disclaimer: Eremedium blogs and videos are for informational purposes only and should not be construed as advice or as a substitute for consulting a physician. It is not a substitute for medical advice or treatment from a healthcare professional.
#pcos #pcostreatment #laparascopicovariandrilling

Mini-Laparoscopic Cholecystectomy with Intraoperative Cholangiogram for Symptomatic Cholelithiasis (Gallstones) - Standard
Authors: Brunt LM1, Singh R1, Yee A2
Published: September 26, 2017
AUTHOR INFORMATION
1 Department of Surgery, Washington University, St. Louis, Missouri
2 Division of Plastic and Reconstructive Surgery, Washington University, St. Louis, Missouri
DISCLOSURE
No authors have a financial interest in any of the products, devices, or drugs mentioned in this production or publication.
ABSTRACT
Minimal invasive laparoscopic cholecystectomy is the typical surgical treatment for cholelithiasis (gallstones), where patients present with a history of upper abdominal pain and episodes of biliary colic. The classic technique for minimal invasive laparoscopic cholecystectomy involves four ports: one umbilicus port, two subcostal ports, and a single epigastric port. The Society of American Gastrointestinal and Endoscopic Surgeons (SAGES) has instituted a six-step strategy to foster a universal culture of safety for cholecystectomy and minimize risk of bile duct injury. The technical steps are documented within the context of the surgical video for (1) achieving a critical view of safety for identification of the cystic duct and artery, (2) intraoperative time-out prior to management of the ductal structures, (3) recognizing the zone of significant risk of injury, and (4) routine intraoperative cholangiography for imaging of the biliary tree. In this case, the patient presented with symptomatic biliary colic due to a gallstone seen on the ultrasound in the gallbladder. The patient was managed a mini-laparoscopic cholecystectomy using 3mm ports for the epigastric and subcostal port sites with intraoperative fluoroscopic cholangiogram. Specifically, the senior author encountered a tight cystic duct preventing the insertion of the cholangiocatheter and the surgical video describes how the author managed the cystic duct for achieving a cholangiogram, in addition to the entire technical details of laparoscopic cholecystectomy.
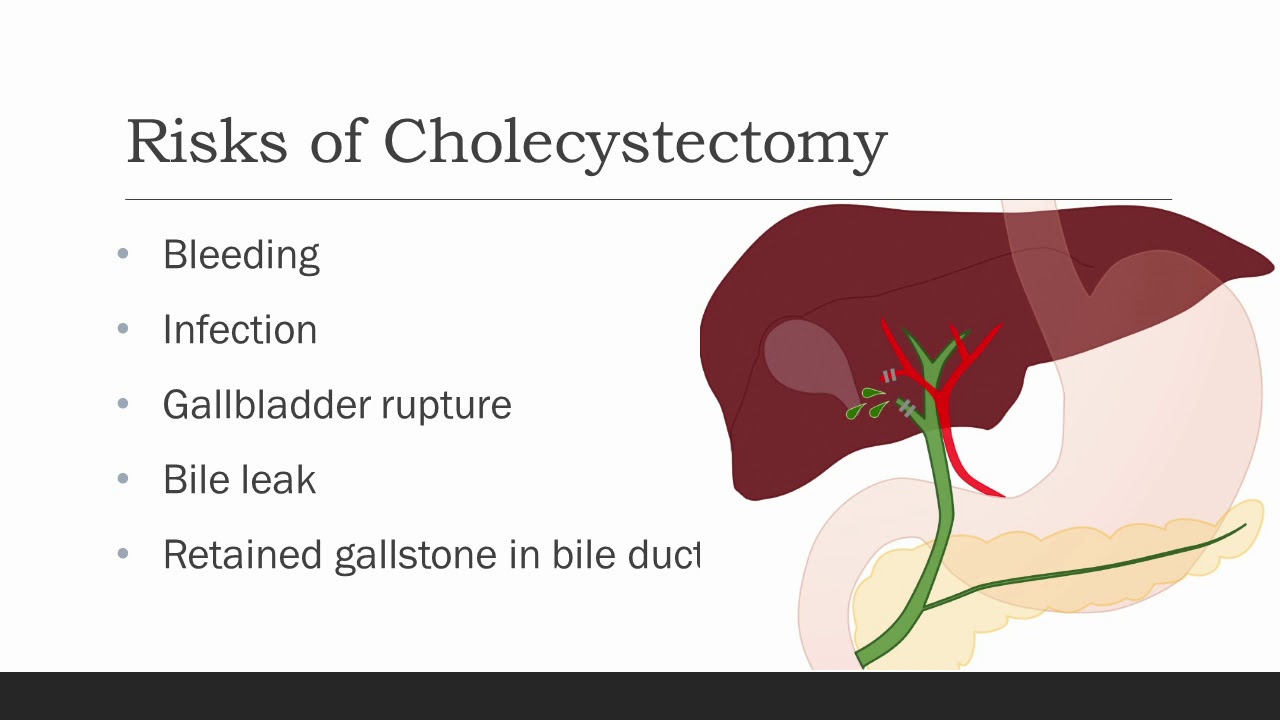
Cholecystectomy means removal of the gallbladder. The most common reasons
your doctor might recommend a cholecystectomy are biliary colic, cholecystitis,
choledocolithiasis, or gallstone pancreatitis. Biliary colic, also known as symptomatic
cholelithiasis, is caused by gallstones, which are hardened deposits of bile. Gallstones are
common in the general population, and gallstones alone are not a reason for gallbladder
removal if they do not cause symptoms. However, sometimes gallstones can get caught at the
neck of the gallbladder, causing pain when the gallbladder contracts against them trying to
release its bile, especially after a fatty meal. With biliary colic, the pain typically resolves within
an hour or so. Occasionally, a stone or some other blockage may prevent the gallbladder from
emptying over a long period of time, causing an increase in pressure and trapped fluid within the
gallbladder. This can cause inflammation and infection of the gallbladder, which we call
cholecystitis. Choledocholithiasis is when there are one or more stones in the bile ducts, which
can cause back up of bile into the liver, and depending on the location of the stones, could
cause pancreatitis, which is inflammation of the pancreas. Other reasons for gallbladder
removal, though less common, are gallbladder polyps and cancer. All of these are reasons for
gallbladder removal.

Visit our website to learn more about using Nucleus animations for patient engagement and content marketing: http://www.nucleushealth.com/?utm_source=youtube&utm_medium=video-description&utm_campaign=appendect-020615
This 3D medical animation depicts the surgical removal of the appendix (appendectomy) using laparoscopic instruments. The surgery animation begins by showing an inflamed appendix (appendicitis), followed by the placement of the laparoscope. Afterward, one can see the surgical device staple, cut and remove the inflamed appendix. Following the removal of the appendix the abdomen is flushed with a sterile saline solution to ensure all traces of infection have been removed.
#laparoscopy #appendix #appendicitis
ANCE00183

UChicago Medicine organ transplant surgeon Dr. Rolf Barth explains a how the laparoscopic donor nephrectomy – also known as the single-port nephrectomy – procedure works to remove an organ donor’s kidney from their body to be transplanted into a recipient. This minimally invasive kidney donor transplant surgery allows living organ donors the get back to their lives more quickly than the traditional approach and leaves them with a nearly invisible scar in the belly button.
Learn more about living kidney donation: https://www.uchicagomedicine.o....rg/conditions-servic

OB_A_1013
3D animation depicting the operating room and initial procedure preparing the patient for a laparoscopic hysterectomy. The patient is prepped and draped in the usual fashion and surrounded by the surgeon and surgical assistants. The skin is elevated, an infraumbilical incision is made, a trocar port is inserted through the incision and the abdomen is insufflated. Finally, a laparoscope is inserted into the port to allow for direct visualization of the uterus and the surgery can begin.
To view more animations and exhibits, visit our medical library: https://www.trialexhibitsinc.c....om/library/multimedi
Contact us on your next case for consulting, trial graphics, animations, medical illustrations or presentation services. 800-591-1123 [a]www.trialex.com[/a]
This video is for reference only. The video may not be otherwise used, reproduced nor modified. For more information to purchase a copy or permission to use this animation on your next case, project, website or TV, contact us at [a]www.trialex.com[/a] or 800-591-1123.
Copyright @ Trial Exhibits, Inc.

This Basic Laparoscopic Surgery: Abdominal Access and Trocar Introduction course will teach you the steps of Laparoscopic Surgery. View the full course for free by signing up on our website: https://www.incision.care/
What is Laparoscopic Surgery:
Laparoscopic surgery describes procedures performed using one or multiple small incisions in the abdominal wall in contrast to the larger, normally singular incision of laparotomy. The technique is based around principles of minimally invasive surgery (or minimal access surgery): a large group of modern surgical procedures carried out by entering the body with the smallest possible damage to tissues. In abdominopelvic surgery, minimally invasive surgery is generally treated as synonymous with laparoscopic surgery as are procedures not technically within the peritoneal cavity, such as totally extraperitoneal hernia repair, or extending beyond the abdomen, such as thoraco-laparoscopic esophagectomy. The term laparoscopy is sometimes used interchangeably, although this is often reserved to describe a visual examination of the peritoneal cavity or the purely scopic component of a laparoscopic procedure. The colloquial keyhole surgery is common in non-medical usage.
Surgical Objective of Laparoscopic Surgery:
The objective of a laparoscopic approach is to minimize surgical trauma when operating on abdominal or pelvic structures. When correctly indicated and performed, this can result in smaller scars, reduced postoperative morbidity, shorter inpatient durations, and a faster return to normal activity. For a number of abdominopelvic procedures, a laparoscopic approach is now generally considered to be the gold-standard treatment option.
Definitions
Developments of Laparoscopic Surgery:
Following a number of smaller-scale applications of minimally invasive techniques to abdominopelvic surgery, laparoscopic surgery became a major part of general surgical practice with the introduction of laparoscopic cholecystectomy in the 1980s and the subsequent pioneering of endoscopic camera technology. This led to the widespread adoption of the technique by the early- to mid-1990s. The portfolio of procedures that can be performed laparoscopically has rapidly expanded with improvements in instruments, imaging, techniques and training — forming a central component of modern surgical practice and cross-specialty curricula [2]. Techniques such as laparoscopically assisted surgery and hand-assisted laparoscopic surgery have allowed the application of laparoscopic techniques to a greater variety of pathology. Single-incision laparoscopic surgery, natural orifice transluminal endoscopic surgery, and minilaparoscopy-assisted natural orifice surgery continue to push forward the applications of minimally invasive abdominopelvic techniques; however, the widespread practice and specific indications for these remain to be fully established. More recently, robotic surgery has been able to build on laparoscopic principles through developments in visualization, ergonomics, and instrumentation.
This Basic Laparoscopic Surgery: Abdominal Access and Trocar Introduction course will teach you:
- How to access the abdomen using an open, closed, and direct optical-entry technique
- Principles underlying safe abdominal insufflation
- The vascular anatomy of the abdominal wall and its implications for trocar placement
- How to introduce trocars into the peritoneal cavity
- The principle of triangulation and how this can be applied to organizing a laparoscopic surgical field
Specific attention is given to these hazards you may encounter:
- Intravascular, intraluminal, or extraperitoneal needle position
- Limitations of a closed introduction technique
- Abdominal surgical history
- Limitations of an open introduction technique
- Optical trocar entry in thin individuals
- Visualization of non-midline structures
- Limitations of direct optical-entry techniques
- Limitations of clinical examination to confirm intraperitoneal insufflation
- Leakage of insufflation gas
These tips are designed to help you improve your understanding and performance:
- Alternative left upper quadrant approach
- Testing Veress needle before use
- Lifting the abdominal wall for Veress needle introduction
- "Hanging-drop test"
- Palmer's test
- Confirming intra-abdominal insufflation
- Subcutaneous tissue retraction
- Anatomy of the umbilicus
- Retraction of abdominal wall fascia
- Finger sweep of anterior abdominal wall
- Lifting the abdominal wall for optical trocar introduction
- Identification of venous bleeding at the end of a procedure
- Identification of inferior epigastric vessels by direct vision
- Peritoneal folds of the anterior abdominal wall
- Transillumination of superficial epigastric vessels
- Infiltration of local anesthetic at port sites
- Aiming of trocars
- Selection of trocar size
- Maintaining direct vision
