- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

HPV causes genital warts and cervical and other anogenital cancers. The HPV vaccine is recommended for girls and women 9 to 26 years of age to reduce infections, but information on safety in pregnant women is limited.
screening and early detection is the key to beating any form of cancer. share this with a friend. you may save a life.
Embolization is a medical advance that shrinks uterine fibroids. One tiny incision allows us to solve the problem quickly, safely and without surgery
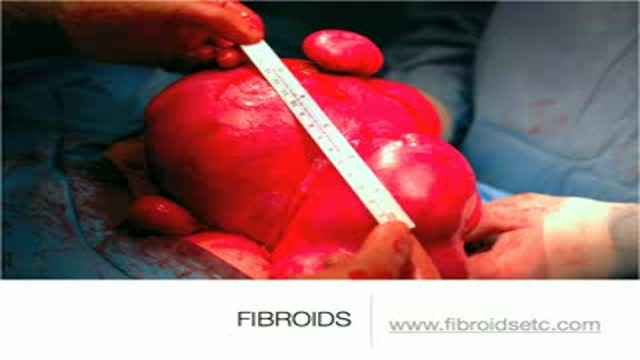
A uterine fibroid (also uterine leiomyoma, myoma, fibromyoma, leiofibromyoma, fibroleiomyoma, and fibroma) (plural of ... myoma is ...myomas or ...myomata) is a benign (non-cancerous) tumor that originates from the smooth muscle layer (myometrium) and the accompanying connective tissue of the uterus. Fibroids are the most common benign tumors in females and typically found during the middle and later reproductive years. While most fibroids are asymptomatic, they can grow and cause heavy and painful menstruation, painful sexual intercourse, and urinary frequency and urgency. Uterine fibroids is the major indication for hysterectomy in the US.[2] Fibroids are often multiple and if the uterus contains too many leiomyomatas to count, it is referred to as uterine leiomyomatosis. The malignant version of a fibroid is uncommon and termed a leiomyosarcoma.


his patient had spilled boiling water on his lower leg a couple days before. This isn't complicated but the teaching points should focus on draining the large blistered areas and attempting to maintain moisture as long as we can so the skin doesn't contract down on itself.

Ingrown Hair Removal Video

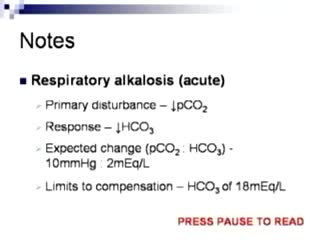
Arterial Blood Gas Sampling

This animated video will run you through the process of nuclear stress test.
http://breatheasthmafree.blog300.com - Asthma Treatments bronchitis - Bronchitis Asthma Home Remedies
Kill Asthma Today!
Natural - Treatment for Asthma
Cure & Revitalise Your Breathing
http://breatheasthmafree.blog300.com
Asthma Treatments bronchitis - Bronchitis Asthma Home Remedies

http://dissolve-kidney-stones-fast.good-info.co/ How To Dissolve Kidney Stone Naturally In Home, Herbs For Kidney Stones, Dissolve Kidney Stones. For thousands of years Amazonian Rainforest tribes have been using the Chanca Piedra plants liquid extract herbs to dissolve kidney stones and gallstones. I found out about this incredible plant, phyllanthus niruri, because I use to suffer from kidney stones. Just like you, I have been in the ER for kidney stones suffering incredible kidney pain. I eventually had to have surgery for relief & removal of the stone. It was a horrendous experience and at that point I knew I had to figure out a way to avoid having another kidney stone in my life! I started doing research and found out the Amazon Rainforest had the remedy! The next time I got kidney stone symptoms I quickly started taking Chanca Piedra tincture drops and it dissolved the stone and I passed it easily. My new mission was to help others suffering from stones. Mine were calcium oxalate, perhaps yours are the same type or uric acid, struvite or cystine. You want the most powerful kidney stone treatment available today and our Kidney Stone Crusher is that product. Make no mistake, if you suffer from stones you need this stone breaker and dissolver passing product! It shrinks and dissolves your stones naturally. No more ER visits, no more painful surgeries, expensive medicine, and no more stents! The added benefit of using our Kidney Stone Crusher is that you will cleanse your liver and kidneys at the same time giving you better digestion, regulate your hormones and purify your blood. Increases urination which is a must for passing stones & cleansing. Our product is all organic, natural and sustainably wildcrafted from the Rainforest in Peru. Works on animals as well, dogs, cats, even alpacas! Click the Buy Button now and get started dissolving your stones. http://dissolve-kidney-stones-fast.good-info.co/

Microsurgical bipolar cautery tonsillectomy compares favorably with traditional techniques in terms of intraoperative bleeding, postoperative pain, otalgia, and hemorrhage. This technique combines the hemostatic advantage of cautery dissection, the excellent visualization achieved by a microscope, and, with the use of a video, greatly improves the physician's ability to teach how to perform a tonsillectomy.
A salivary gland stone -- also called salivary duct stone -- is a calcified structure that may form inside a salivary gland or duct. It can block the flow of saliva into the mouth. The majority of stones affect the submandibular glands located at the floor of the mouth.
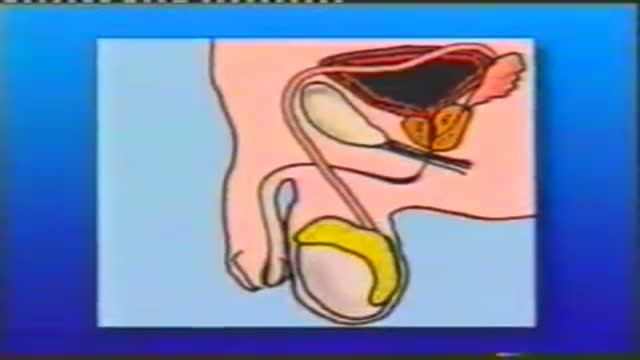
Basic well-male examination of the genitals and digital rectal exam.

Drainage of Pus from a Dental Abscess
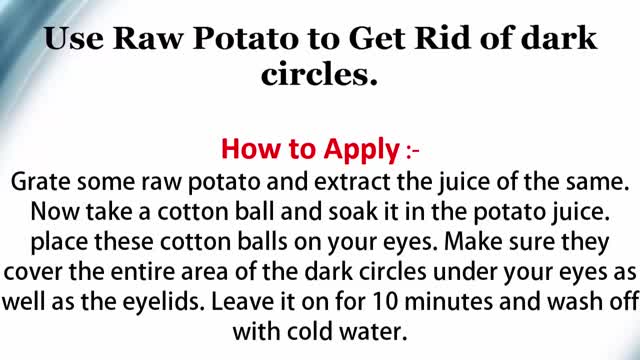
Dark Circles around Eyes
Lichen sclerosus is a skin condition that mainly affects the genital skin (vulva) in women and the penis in men. It most commonly occurs in middle-aged women. Symptoms may include itch, soreness, and changes in the appearance of affected skin.

A cervical rib in humans is an extra rib which arises from the seventh cervical vertebra. Sometimes known as "neck ribs", their presence is a congenital abnormality located above the normal first rib. A cervical rib is estimated to occur in 0.2% (1 in 500 people) to 0.5% of the population.
