- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
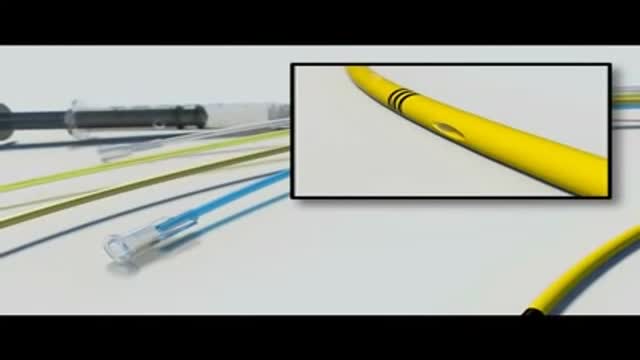
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Clinical Examination - Gait, Arms, Legs, Spine

A video showing how to insert the Intra Uterine Device (IUD)
Recto-vaginal medical examination

Watch that video of Popping Huge Epidermoid Cyst

Watch that video of MRI Scans Human Body Internal Organs During Sex
ADH's job is to act on the kidneys to promote water reabsorption. In this lesson, we'll compare and contrast diabetes insipidus, or DI, in which there is too little ADH, and syndrome of inappropriate antidiuretic hormone secretion , or SIADH, in which there is too much ADH.

A stepwise approach to the causes and diagnosis of Anaemia in clinical practice. This presentation includes the all important concept of the Reticulocyte production index. Discussion of Hereditary and acquired causes of Anaemia has been included in detail.
An old video showing how to give an enema
http://www.wss4m.com/vb
Any independent vertical movement of the transducer or the patient will affect the hydrostatic column of this fluid-filled system and thus alter the pressure measurements. At some time before or after PAC insertion, the system must therefore be zeroed to ambient air pressure. The reference point for this is the midpoint of the left atrium (LA), estimated as the fourth intercostal space in the midaxillary line with the patient in the supine position. With the transducer at this height, the membrane is exposed to atmospheric pressure, and the monitor is then adjusted to zero. Calibration Once zeroed, the monitoring system must be calibrated for accuracy. Currently, most monitors perform an automated electronic calibration. Two methods are used to manually calibrate and check the system. If the catheter has not been inserted, the distal tip of the PAC is raised to a specified height above the LA. For example, raising the tip 20 cm above the LA should produce a reading of approximately 15 mm Hg if the system is working properly (1 mm Hg equals 1.36 cm H 2 O). Alternatively, pressure can be applied externally to the transducer and adjusted to a known level using a mercury or aneroid manometer. The monitor then is adjusted to read this pressure, and the system is calibrated. Dynamic tuning Central pressures are dynamic waveforms (ie, they vary from systole to diastole) and thus have a periodic frequency. To monitor these pressures accurately, the system requires an appropriate frequency response. A poorly responsive system produces inaccurate pressure readings, and differentiating waveforms (eg, PA from pulmonary capillary wedge pressure [PCWP]) can become difficult. When signal energy is lost, the pressure waveform is dampened. Common causes of this are air bubbles (which are compressible), long or compliant tubing, vessel wall impingement, intracatheter debris, transducer malfunction, and loose connections in the tubing. A qualitative test of the frequency response is performed by flicking the catheter and observing a brisk high-frequency response in the waveform. After insertion, the system can be checked by using the rapid flush test. When flushed, an appropriately responsive system shows an initial horizontal straight line with a high-pressure reading. Once the flushing is terminated, the pressure drops immediately, which is represented by a vertical line that plunges below the baseline. A brief and well-defined oscillation occurs, followed by return of the PA waveform. A dampened system will not overshoot or oscillate, and causes a delay in returning to the PA waveform.
Cardiovascular surgery basically treats a number of diseases and medical disorders that affect your heart and the network of arteries and veins connecting it to every part of the body. https://goo.gl/iphEi9

Watch that video of Huge 132 lbs Testicles Tumor Removal Surgery
mply put, relapses, also known as flare ups, or (MS) attacks are new or worsening MS symptoms. But there is a concrete definition used by healthcare providers to identify MS attacks. To be considered an MS relapse: Old symptoms of MS must have become worse or new symptoms appeared.
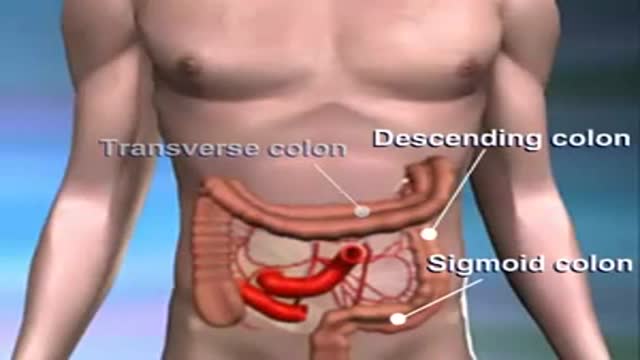
Colon cancer usually begins as a non-cancerous growth. If caught early enough, it can be safely removed with little to no complications.
http://tinnitus-solution.info-pro.co --- Ear Infection, Loud Ringing In Ears, Tinnitus Suicide, Ear Is Ringing, Tinnitus One Ear, Tinnitus. Do you suddenly get up in the middle of the night hearing strange noises? Yes it can definitely be frightening, more so when you cannot find the source. Now consider for a moment that these sounds are coming from within you. Most people would be stunned to know that. Many of us do not even know that our internal organs can make sounds. Let us try to see whether you actually heard these noises or not, and if you did, where did they come from. Now before anything, let us get this straight - yes, you actually heard those noises. No, they are not a result of a creative mind that imagined things in slumber. But having said that, it is also true that there is indeed no source of the sounds you heard. So what is it? Confused? This is a classic case of tinnitus. What is tinnitus? What you experienced last night (or did you just get up from sleep and switch on the computer) is a classic case of tinnitus. This is a medical condition wherein a person hears all kinds of strange clicking, ringing, buzzing, whistling or hissing sounds within the ear. What's so worrisome about this condition for a lot of people is that, there's actually no physical source of these sounds. What makes it even worse is that, no one else seems to hear them. Frankly, these people cannot be really blamed. Naturally, if you cannot see where the sound is coming from, and if you keep hearing it, you are bound to get worried. In tinnitus, the sounds a person hears are actually perceptions. Since there's no actual source, they are often referred to as "phantom noises". Will it help you if you knew that about 8% of all people in the US suffer from tinnitus? Perhaps not, but at least now you know that you are not alone who hears these strange noises. Cure tinnitus. this simple, but effective system to erasing Tinnitus out of your life for good has now helped cure over 105,302 people of all the frustrating ringing, hissing, buzzing. Even if you’ve tried every single tinnitus treatment or remedy under the sun. 100% natural tinnitus cure click here: http://tinnitus-solution.info-pro.co

Men and women have anatomical differences when it comes to genitals, but orgasms are fundamentally very similar. The female orgasm lasts longer than the male, ranging about 20 seconds compared to 3 to 10 seconds, but men do experience more orgasms.

SINUS LIFT SURGERY surgical procedure which aims to increase the amount of bone in the posterior maxilla (upper jaw bone), in the area of the premolar and molar teeth, by lifting the lower Schneiderian membrane (sinus membrane) and placing a bone graft.

This video demonstrates the use of an episiotomy to facilitate vaginal delivery of a baby

Doctor shares tips on what to expect after a cancer diagnosis
A hemangioma (he-man-jee-O-muh) is a birthmark that most commonly appears as a rubbery, bright red nodule of extra blood vessels in the skin. A hemangioma grows during the first year of life, and then recedes over time. A child who had a hemangioma during infancy usually has little visible trace of the growth by age 10.
