- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
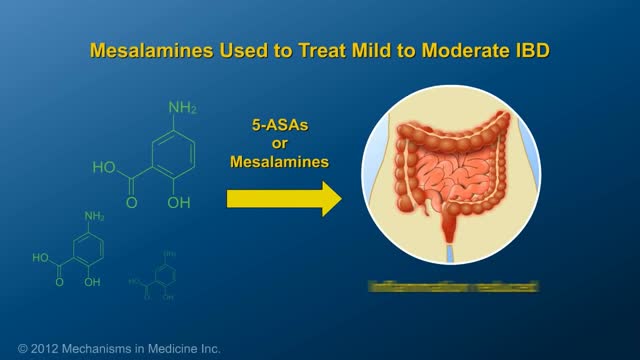
This animation describes risks of inflammatory bowel disease (IBD) and risks/benefits of medication (5-ASAs, steroids, immunomodulators, & biologics).

Thousands of Whiteheads! Why Do I Get Them?
Dilation and curettage (D&C) is a procedure to remove tissue from inside your uterus. Doctors perform dilation and curettage to diagnose and treat certain uterine conditions — such as heavy bleeding — or to clear the uterine lining after a miscarriage or abortion. In a dilation and curettage — sometimes spelled "dilatation" and curettage — your doctor uses small instruments or a medication to open (dilate) your cervix — the lower, narrow part of your uterus. Your doctor then uses a surgical instrument called a curette to remove uterine tissue. Curettes used in a D&C can be sharp or use suction

Female breast exam video

Anatomical snuff box tenderness due to probable scaphoid wrist bone fracture.

Chalazions are extremely common, and having a sound surgical technique to drain a chalazion is a fundamental in general ophthalmology and oculoplastic surgery. I believe one of the biggest downfalls in treating chalazions is inadequate local anesthetic. Please that both the outer and inner surface to the eyelid need to receive local anesthesia to make the patient totally comfortable. It is important to be careful in delivering the local anesthetic and making sure you have control of the head position, and the position of your needle is bent to minimize any possibility of contact with the globe.

Down’s Syndrome Twins Are One In A Million

NURSING VIDEO ACTUAL CATHETERIZATION PROCEDURE OF MALE. FULL LENGTH VERSION Clear quality photography. This video provides an excellant clinical view of the entire procedure.
Actual Footage of Cell Division (Kidney Cells) see more http://www.kidneymy.com/

After 11 years of my work on my new migraine surgery, I start to do migraine surgery in all 4 principal places - places # 1 (STA) both sides, and places # 3 - Occipital artery also from both sides. You can see my first patients; he had bifrontal migraine headaches and daily chronic headaches in occipital area and the top of the head. On 30 September I sutured the occipital artery from both sides, and on 2 October I sutured STA in places # 1 from both sides. www.alisultaneh.8m.com

Watch that video to know How to Insert Enema
Acute kidney failure occurs when your kidneys suddenly become unable to filter waste products from your blood. When your kidneys lose their filtering ability, dangerous levels of wastes may accumulate, and your blood's chemical makeup may get out of balance. Acute kidney failure — also called acute renal failure or acute kidney injury — develops rapidly over a few hours or a few days. Acute kidney failure is most common in people who are already hospitalized, particularly in critically ill people who need intensive care. Acute kidney failure can be fatal and requires intensive treatment. However, acute kidney failure may be reversible. If you're otherwise in good health, you may recover normal or nearly normal kidney function.
USMLE Step 2 CS - BPH - This is just preview video. To get full access please visit our website : www.usmletutoring.com

The products of a surgical abortion.

Pulmonary edema is almost always treated in the emergency room or hospital. You may need to be in an intensive care unit (ICU). Oxygen is given through a face mask or tiny plastic tubes are placed in the nose. A breathing tube may be placed into the windpipe (trachea) so you can be connected to a breathing machine (ventilator) if you cannot breathe well on your own. The cause of edema should be identified and treated quickly. For example, if a heart attack has caused the condition, it must be treated right away. Medicines that may be used include: Diuretics that remove excess fluid from the body Medicines that strengthen the heart muscle, control the heartbeat, or relieve pressure on the heart
http://www.vaginal-ultrasound.com A demonstration of a vaginal ultrasound.
Scientists reveal how LSD alters your mind.

Nipple Sensation After Breast Augmentation
Lichen sclerosus is a skin condition that mainly affects the genital skin (vulva) in women and the penis in men. It most commonly occurs in middle-aged women. Symptoms may include itch, soreness, and changes in the appearance of affected skin.

Pomeroy Tubal Ligation during a C-Sections
