- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Watch that Female Recto-vaginal Exam Video
https://www.youtube.com/watch?v=Uc6ZotU5mxA

ectal exam is an internal examination of the rectum such as by a physician or other healthcare professional.
The digital rectal examination (DRE, Latin palpatio per anum or PPA) is a relatively simple procedure. The patient is placed in a position where the anus is accessible and relaxed (lying on the side, squatting on the examination table, bent over the examination table, etc). The physician inserts a gloved and lubricated finger into the rectum through the anus and palpates the insides.
The DRE is inadequate as a screening tool for colorectal cancer because it examines less than 10% of the colorectal mucosa; colonoscopy is preferred. However, it's an important part of a general examination, as many tumors or other diseases are made manifest in the distal part of the rectum.
This examination may be used: * for the diagnosis of rectal tumors and other forms of cancer; * in males, for the diagnosis of prostatic disorders, notably tumors and benign prostatic hyperplasia; * for the diagnosis of appendicitis or other examples of an acute abdomen (i.e. acute abdominal symptoms indicating a serious underlying disease); * for the estimation of the tonicity of the anal sphincter, which may be useful in case of fecal incontinence or neurologic diseases, including traumatic spinal cord injuries; * in females, for gynecological palpations of internal organs * for examination of the hardness and color of the feces (ie. in cases of constipation, and fecal impaction); * prior to a colonoscopy or proctoscopy. * to evaluate haemorrhoids
The DRE is frequently combined with an FOBT (fecal occult blood test), which may be useful for diagnosing the etiology of an anemia and/or confirming a gastrointestinal bleed.
Sometimes proctoscopy may also be part of a rectal examination.

Normal Vaginal Delivery

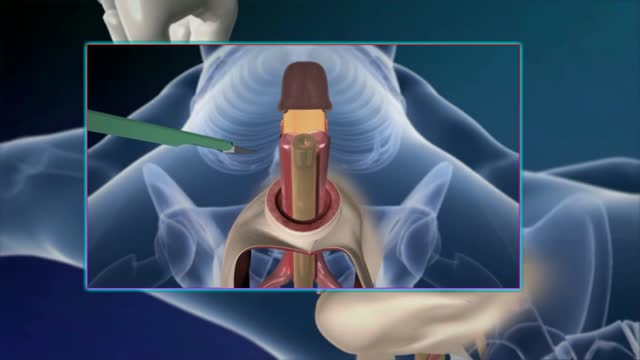
http://www.proctoscopeexam.com This is a demonstration of a proctoscope examination of the rectum.

Female Circumcision - FGM Female Genital Mutilation - female circumcision ختان الاناث - женское обрезание - circuncisão feminina - 女性割禮 - besnijdenis - babae pagtutuli - l'excision - κλειτοριδεκτομή - הנקבה מולה - sunat perempuan - circoncisione femminile - 女子割礼 - 여성 할례 - la circuncisión femenina - หญิง circumcision - kadın sünnet - жіноче обрізання For More read at World Health Organization web site : http://www.who.int/topics/female_genital_mutilation/en/index.html other sites : http://en.wikipedia.org/wiki/Female_genital_cutting

Orgasmic childbirth is a new variant of water birth delivery.

http://www.hypodermic-injection.com This is a demonstration of an IM hypodermic injection administered in the gluteus maximus muscle. The patient is in the prone position.

Physical exam by a urologist including kidney, testicular and prostate exam.

Surgical abortion using the dilatation and curretage technique.

Proctoscope rectal examination

There are lots of fallacies about the missionary position being the best position for getting pregnant. With the woman on her back and her partner on top, it is thought that gravity will assist the sperm to swim upwards towards the egg.


This video demonstrates the management of a large abscess in the emergency department. This abscess probably began as a sebaceous cyst that became infected.

this video shows how the child circumcision is easy and safe with alisklamp
Sex reassignment surgery for male-to-female involves reshaping the male genitals into a form with the appearance of, and, as far as possible, the function of female genitalia. Prior to any surgeries, patients usually undergo hormone replacement therapy (HRT), and, depending on the age at which HRT begins, facial hair removal. There are associated surgeries patients may elect to, including facial feminization surgery, breast augmentation, and various other procedures

Watch that Female to Male Gender Changing Surgery

Watch that video of MRI Scans Human Body Internal Organs During Sex

Dr Chris Steele demonstrates a breast examination on a live model. This shows how to check yourself for early signs of tumours, cysts and other symptoms of breast cancer.

Proctoscopy in Jackknife Position for examination of the rectum
