- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
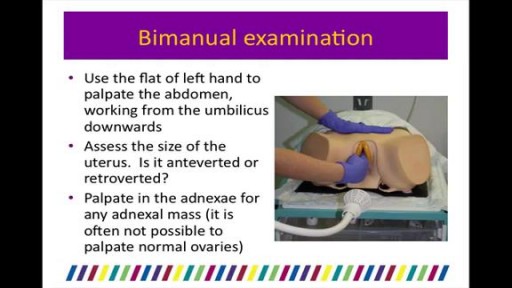
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
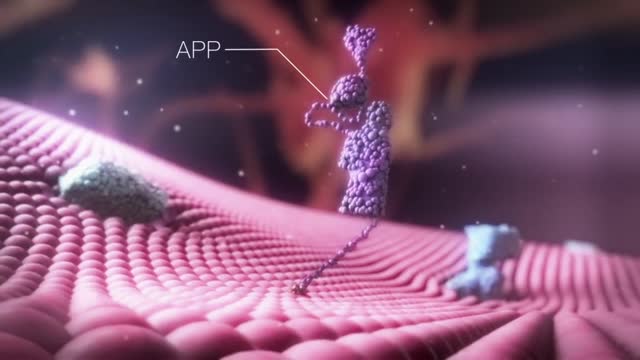
The cell membrane is selectively permeable to ions and organic molecules and controls the movement of substances in and out of cells. The basic function of the cell membrane is to protect the cell from its surroundings. It consists of the phospholipid bilayer with embedded proteins.

If you are self-conscious because you have missing teeth, wear dentures that are uncomfortable or don't want to have good tooth structure removed to make a bridge, talk to your dentist to see if dental implants are an option for you. Dental implants are a popular and effective way to replace missing teeth and are designed to blend in with your other teeth. They are an excellent long-term option for restoring your smile. In fact, the development and use of implants is one of the biggest advances in dentistry in the past 40 years. Dental implants are made up of titanium and other materials that are compatible with the human body. They are posts that are surgically placed in the upper or lower jaw, where they function as a sturdy anchor for replacement teeth.
Anatomy of Love
The cause of HELLP syndrome is unknown, but there are certain factors that may increase your risk of developing it. Preeclampsia is the greatest risk factor. This condition is marked by high blood pressure and swelling, and it typically occurs during the last trimester of pregnancy.
Wilms tumor, also known as nephroblastoma, is a cancer of the kidneys that typically occurs in children, rarely in adults. It is named after Dr. Max Wilms, the German surgeon (1867–1918) who first described it. Approximately 500 cases are diagnosed in the U.S. annually.

Silicone Brow Suspension of Eye Lid

Have you watched a surgery on a horse before?

For both DCIS and invasive cancer, radiation therapy to the remaining breast tissue is generally recommended after surgery. A lumpectomy may also be called breast-conserving surgery, a partial mastectomy, quadrantectomy, or a segmental mastectomy. A mastectomy is the surgical removal of the entire breast.

Watch that video of an Ingrown Hair Causes Huge Tumor in a Man's Stomach
Huge Abscess On Man's Jaw surgery

examination of the recturm

#ComprehensiveClinicalClass
History, Examination and Management of Hernia
Mentor: Dr. Nishanth, Consultant Surgeon, Bengaluru.
THE WHITE ARMY
To make studies more interesting and enjoyable, we are constantly trying to share most important tables, charts, diagrams, mnemonics, scoring systems, diagnostic criterias, motivating quotes and other useful study materials on
ANDROID APP - All in 1 Free Medical Education App for Medicos
https://play.google.com/store/....apps/details?id=com.
INSTAGRAM PAGE
@the_whitearmy
https://www.instagram.com/the_whitearmy/
TELEGRAM GROUP
PDFs, PPTs and other study materials stored for easy, convenient access and download.
https://t.me/whitearmyofmedicos
Anyone interested to present clinical cases, willing to join whatsapp discussion group, can send a mail to whitearmyofmedicos@gmail.com
#StudyManiaInSocialMedia
#HelpOthersToHelpOurselves
#StudyEnjoyingEnjoyStudying
DISCLAIMER
THE WHITE ARMY does not own or claim to own any of the media used in the following video/stream. The media belong to their respective owners who may have copyright over them.The media have been taken from various sources and are used for medical educational purposes only. The following video/stream may contain images that may not be suitable for all audiences, viewer discretion is advised.

Ganglion cysts are noncancerous lumps that most commonly develop along the tendons or joints of your wrists or hands. They also may occur in the ankles and feet. Ganglion cysts are typically round or oval and are filled with a jellylike fluid. Small ganglion cysts can be pea-sized, while larger ones can be around an inch (2.5 centimeters) in diameter. Ganglion cysts can be painful if they press on a nearby nerve. Their location can sometimes interfere with joint movement. If your ganglion cyst is causing you problems, your doctor may suggest trying to drain the cyst with a needle. Removing the cyst surgically also is an option. But if you have no symptoms, no treatment is necessary. In many cases, the cysts go away on their own.
Basic well-male examination of the genitals and digital rectal exam.
Watch that Recto vaginal Exam Video

This patient presented to the ER for umbilical pain and had a history of umbilical hernia. He was concerned about the possibility of incarceration of the hernia.
In this video we explain how the clinical exam helps to differentiate a simple painful hernia from an incarcerated one.
***Thanks to the patient for sharing his history and exam with YouTube world***
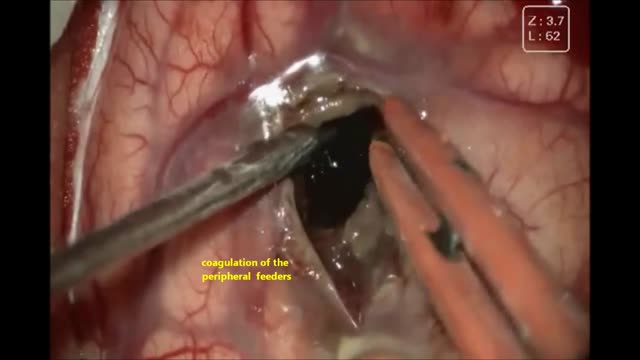
This 13 yrs young girl has had left temporo parietal cavernous angioma ,she came with acute bleed with raised ICT ,aphasia ,right hemiparesis ,leision was excised microsurgically with excellent out come
A video showing how to catheter the male urethra
Alzheimer's is the most common form of dementia, a general term for memory loss and other intellectual abilities serious enough to interfere with daily life. Alzheimer's disease accounts for 60 to 80 percent of dementia cases. Alzheimer's is not a normal part of aging, although the greatest known risk factor is increasing age, and the majority of people with Alzheimer's are 65 and older. But Alzheimer's is not just a disease of old age. Up to 5 percent of people with the disease have early onset Alzheimer's (also known as younger-onset), which often appears when someone is in their 40s or 50s.

Chickenpox (varicella) is a viral infection that causes an itchy rash with small, fluid-filled blisters. Chickenpox is highly contagious to people who haven't had the disease or been vaccinated against it. Before routine chickenpox vaccination, virtually all people had been infected by the time they reached adulthood, sometimes with serious complications. Today, the number of cases and hospitalizations is down dramatically. For most people, chickenpox is a mild disease. Still, it's better to get vaccinated. The chickenpox vaccine is a safe, effective way to prevent chickenpox and its possible complications.
