- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Bandaging a freshly above the knee amputated limb

A very funny song made by the staff of the Ob/Gyn Gangnam style

An esophageal stent is a flexible mesh tube, approximately 2cm (3/4 inch) wide, and is placed through the constricted area of your esophagus (food tube) to allow food and beverages to pass from your mouth to your stomach for digestion and absorption of nutrients.

Intradermal Injection

A lot of women want to know what type of vaginal discharge is normal during pregnancy, and when you're not pregnant. So let's start out by talking about what's normal when you're not pregnant. It's normal to have about 1/2 teaspoon to 1 teaspoon of whitish, creamy, tannish discharge on most days of your cycle in between periods, with the exception of the time of ovulation. Actually, around the time of ovulation, it's normal to notice the discharge becoming more slippery and clear, almost like egg whites. And this is actually a sign that you can watch for to know when you're ovulating. And if you're seeing this type of discharge and you're trying to have a baby, then you should start to time intercourse with ovulation to increase your chances of conceiving.

Tonsillectomy 3D Animation
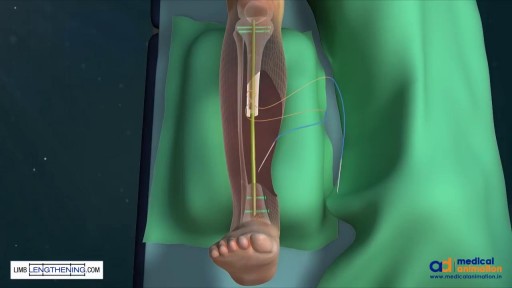
Tibial Bone Transport Over an Intramedullary Nail Using Cable and Pulleys

Brachytherapy or localized radiation treatment can be used in certain patients with breast cancer. Depending on tumor size and other factor, physicians may use APBI or accelerated partial breast irradiation. Dr. Elizabeth Tapen, a radiation oncologist, reviews brachytherapy for breast cancer.

Grape Jelly Abscess on the Butt
From across the room, using controls and pedals—pediatric surgeons at Golisano Children’s Hospital are now able to operate on patients without even touching them. “It allows performances of deep surgeries in the pelvis or abdomen through tiny, little incisions as opposed to a traditional, large incision to get access to the areas where urologists often operate,” explained Dr. Rahman Abd-El-Barr, a pediatric urologist with Golisano Children’s Hospital of Southwest Florida.
The DaVinci robot is a robotic platform that allows surgeons to do minimally invasive surgery, leaving patients with smaller incisions and a quicker recovery. “This is important because it allows us to minimize recovery time, pain, bleeding with surgery, and especially with kids, it helps them to get back on their feet right away,” he said.
So when high school athlete, Reagan Rebeor found out she needed to have kidney surgery, she decided to have it robotically. “Thankfully, I did that because if not, I would have had a long scar down my stomach instead of small holes, small incisions. I had pain for three days, three or four days. Then after that, I was fine,” she said.
While it’s not an option for all pediatric surgeries, doctors say it can be very beneficial for teenage and adult patients needing reconstructive surgery. An option that allows patients a quicker and easier recovery.
View More Health Matters video segments at LeeHealth.org/Healthmatters/
Lee Health in Fort Myers, FL is the largest network of health care facilities in Southwest Florida and is highly respected for its expertise, innovation and quality of care. For more than 100 years, we’ve been providing our community with personalized preventative health services and primary care to highly specialized care services and robotic assisted surgeries. Lee Health - Caring People. Inspiring Care.
Visit LeeHealth.org

Watch that video to know How to Get Rid of Stretch Marks Fast - Get Rid of Stretch Marks Naturally

Ankylosing spondylitis is an inflammatory disease that, over time, can cause some of the vertebrae in your spine to fuse. This fusing makes the spine less flexible and can result in a hunched-forward posture. If ribs are affected, it can be difficult to breathe deeply. Ankylosing spondylitis affects men more often than women. Signs and symptoms typically begin in early adulthood. Inflammation also can occur in other parts of your body — most commonly, your eyes. There is no cure for ankylosing spondylitis, but treatments can lessen your symptoms and possibly slow progression of the disease.

The surgical procedure uses your own fat, so it is the most natural way to augment your buttocks. Over the last few years, the buttocks have received more press coverage than ever before. People of all ages and body types are having the Brazilian Butt Lift procedure.
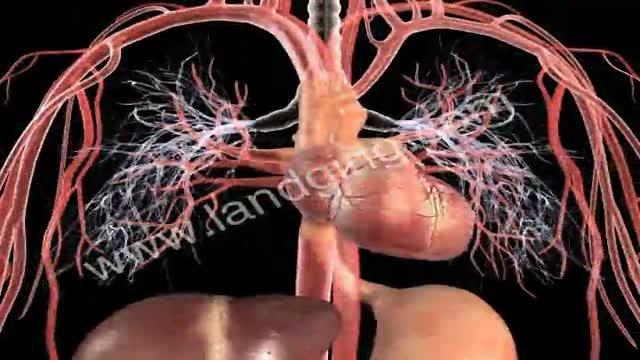
http://www.landging.com/circulatory-system-animation-cardiology.html
This circulatory system animation demonstrates cardiology mechanism of action and pharmacology in 3d.
M. D. Anderson Cancer Center provides a basic education on cancer.
Hepatitis B is a serious disease caused by a virus that attacks the liver. The virus, which is called hepatitis B virus (HBV), can cause lifelong infection, cirrhosis (scarring) of the liver, liver cancer, liver failure, and death. Hepatitis B vaccine is available for all age groups to prevent HBV infection.

today we talk about Amniotic fluid during your pregnancy! Looking forward to your comments.

Uterine rupture is usually when the scar from your previous caesarean section tears open. Though it's uncommon, you should be aware of this risk, particularly if you're thinking about giving birth vaginally next time. It's possible for your scar to gape slightly while you're pregnant (scar dehiscence).
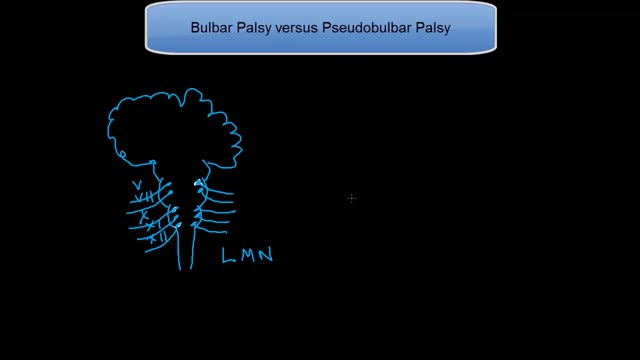
This tutorial explains the difference in mechanisms between the 2 palsies. Bulbar palsy is a lower motor neuron condition and pseudobulbar palsy is an upper motor neuron condidtion.
There’s a strange, mysterious world inside us, an alien-looking environment that turns the food we eat into nutrients that keep us alive. Michael Mosley swallows a camera to take a closer look.
