- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
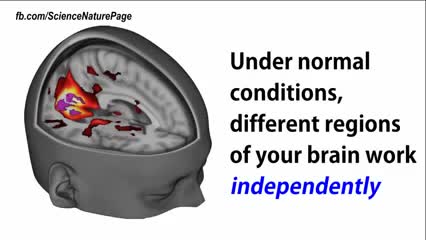
Scientists reveal how LSD alters your mind.
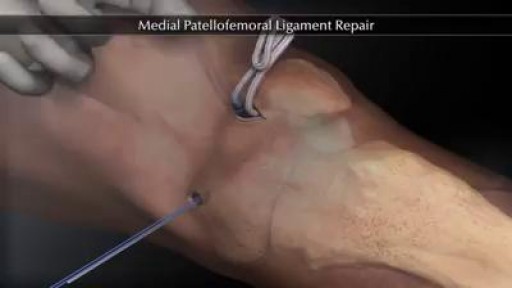
The medial patellofemoral ligament (MPFL) helps to keep the kneecap centered along the front of the knee, so that it tracks well during knee movements. MPFL injuries typically occur during a forceful traumatic kneecap dislocation. This injury is most common among young, active females. Depending on the severity of an MPFL injury, treatment may involve surgical reconstruction, followed by physical therapy. Physical therapists design treatment programs for individuals with MPFL injuries to help them gently restore their knee strength and function.
What Causes Chest Pain ?

Watch that video to know What is Vaginal Discharge and how to Get Rid of it ?
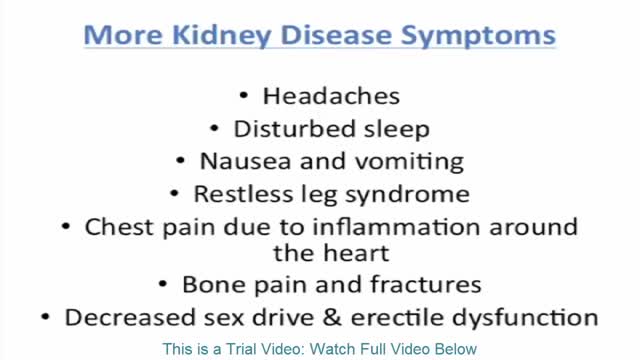
Signs and symptoms of chronic kidney disease develop over time if kidney damage progresses slowly. Signs and symptoms of kidney disease may include: Nausea Vomiting Loss of appetite Fatigue and weakness Sleep problems Changes in how much you urinate Decreased mental sharpness Muscle twitches and cramps Swelling of feet and ankles Persistent itching Chest pain, if fluid builds up around the lining of the heart Shortness of breath, if fluid builds up in the lungs High blood pressure (hypertension) that's difficult to control Signs and symptoms of kidney disease are often nonspecific, meaning they can also be caused by other illnesses. Because your kidneys are highly adaptable and able to compensate for lost function, signs and symptoms may not appear until irreversible damage has occurred.

Pulmonary edema is almost always treated in the emergency room or hospital. You may need to be in an intensive care unit (ICU). Oxygen is given through a face mask or tiny plastic tubes are placed in the nose. A breathing tube may be placed into the windpipe (trachea) so you can be connected to a breathing machine (ventilator) if you cannot breathe well on your own. The cause of edema should be identified and treated quickly. For example, if a heart attack has caused the condition, it must be treated right away. Medicines that may be used include: Diuretics that remove excess fluid from the body Medicines that strengthen the heart muscle, control the heartbeat, or relieve pressure on the heart
Watch that video to know How to Get Pregnant With Twins Naturally

Finger Abscess Incision and Drainage. Digital block with drainage.

A walk through of an interactive about male to female sex reassignment surgery.
The Epley maneuver is a series of movements, normally carried out on a person by a doctor, to relieve the symptoms of BPPV. Research has found it to be an easy, safe, and effective treatment for the condition in both the long- and short-term. The Epley maneuver is sometimes called the particle repositioning maneuver or the canalith repositioning maneuver. These names are used because the maneuver involves a series of movements that help to reposition crystals in a person's ear that may cause feelings of dizziness. Repositioning the crystals helps to relieve the person's dizziness and nausea.
Correcting fgm https://oddafrica.com/videos/female-genital-mutilation-in-africa/

Majority of patients these days prefer PCNL ( Minimal Invasive Telescopic removal of kidney stones broken with lithoclast, removed through a button hole incision ). This patient with a big stone in the pelvis of the kidney wanted it open only so I did an open pyelolithotomy for this patient after a long time as I use to do it in routine in the past. Except for the long incision and scar as compared to PCNL the recovery time was the same and patient went home third day happily walking and eating.
Ever wonder How Male to Female Trans'Gender Surgery works?
all you need to know about the female orgasm

Gynecological Examination

Thai Medical Vacation is the largest medical tours facilitator in Asia. Solutions include Plastic surgery in Thailand,Knee and hip replacements in Thailand,fertility solutions Thailand,cancer therapy in Thailand and stem cell treatments in Thailand, dentistry abroad,and traditional chinese and thai treatments along with orthopedic joint treatments in Thailand

Childbirth (also called labour, birth, partus or parturition) is the culmination of a human pregnancy or gestation period with the birth of one or more newborn infants from a woman's uterus. The process of normal human childbirth is categorized in three stages of labour: the shortening and dilation of the cervix, descent and birth of the infant, and birth of the placenta. In many cases, with increasing frequency, childbirth is achieved through caesarean section, the removal of the neonate through a surgical incision in the abdomen, rather than through vaginal birth. In the U.S. and Canada it represents nearly 1 in 3 (31.8%) and 1 in 4 (22.5%) of all childbirths, respectively.
USMLE Step 2 CS - BPH - This is just preview video. To get full access please visit our website : www.usmletutoring.com
Vaginismus is unique because it may result from a combination of physical or non-physical causes—or seem to have none at all.

"The act of cutting off the prepuce or foreskin of males, or the internal labia of females." Webster's Revised Unabridged Dictionary (1913)
