- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
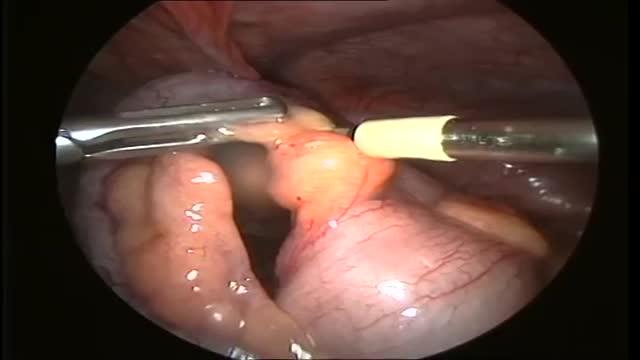
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Colorectal cancer (also known as colon cancer, rectal cancer or bowel cancer) is the development of cancer in the colon or rectum (parts of the large intestine). It is due to the abnormal growth of cells that have the ability to invade or spread to other parts of the body. People with HNPCC tend to develop colon cancer before age 50. Familial adenomatous polyposis (FAP). FAP is a rare disorder that causes you to develop thousands of polyps in the lining of your colon and rectum. People with untreated FAP have a greatly increased risk of developing colon cancer before age 40.

Root canal is a treatment to repair and save a badly damaged or infected tooth instead of removing it. The term "root canal" comes from cleaning of the canals inside a tooth's root. Decades ago, root canal treatments often were painful. With dental advances and local anesthetics, most people have little if any pain with a root canal. In fact, it's probably more painful living with a decayed tooth. Root canal alternatives include extracting the damaged tooth and replacing it with a dental implant, bridge or removable partial denture.

Ways to Help Pregnant Women Dilate HD

Watch that video of Removing Gauze From a Spider's Bite

Most folks remember puberty – and not always in a good way. It can be an awkward stage of budding breasts, unwanted hair, acne and unexpected body odor. Puberty, when a child undergoes physical changes and becomes sexually mature, typically begins around age 8 in girls and age 9 in boys. But imagine, say, a 6- or 7-year-old undergoing such changes? Studies are showing that the onset of puberty for both boys and girls is occurring earlier and earlier, a phenomenon defined as precocious puberty. A study published in Pediatrics in 2010 found that among a population of 1,200 American girls, about 23 percent of African-Americans,15 percent of Latinas and 10 percent of Caucasian girls had begun puberty (marked by breast development) at age 7. In 2012, another study published in Pediatrics found that puberty in American boys – measured by testicular enlargement and pubic hair growth – was beginning six months to two years earlier than what research in previous decades had documented, particularly among African-American children.
One thing we do know: We can live without it, without apparent consequences. Appendicitis is a medical emergency that requires prompt surgery to remove the appendix. Left untreated, an inflamed appendix will eventually burst, or perforate, spilling infectious materials into the abdominal cavity.

Surgical Examination of an ulcer in a proper way
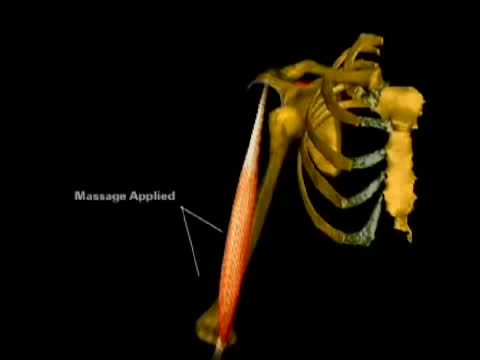
This is an animation of the biomechanics involved in relocating a dislocated shoulder.

The fascinating way doctors insert a stent when there is plaque buildup in an artery.

M. Patrick Lowe, MD, renowned robotic surgeon and gynecologic oncologist at Northwestern Memorial Hospital, will demonstrate the use of robotic surgery to treat endometrial cancer.
Dr. Lowe, director of the robotics and minimally invasive surgical program for the Division of Gynecologic Oncology at Northwestern University's Feinberg School of Medicine, was among the early adopters of robotics to treat gynecologic malignancies, citing precision, improved dexterity and superior patient outcomes among the benefits.
"Women diagnosed with a gynecologic malignancy want the shortest route leading back to a degree of normalcy post treatment," says Lowe. "Robotic surgery offers the path of least resistance, combining shorter recovery times with superior outcomes."
Anemia is a condition in which the body does not have enough healthy red blood cells. Red blood cells provide oxygen to body tissues. There are many types of anemia. Pernicious anemia is a decrease in red blood cells that occurs when the intestines cannot properly absorb vitamin B12.
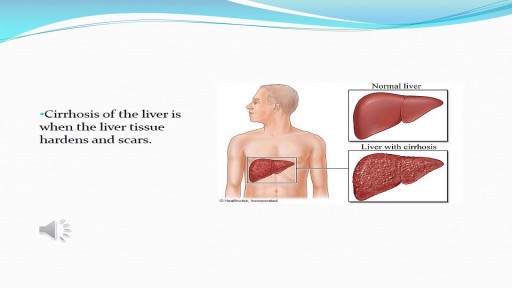
In the United States, end-stage liver disease (ESLD) is the 12th leading cause of death and the 7th leading cause of death in people between the ages of 25 and 64 years. Complications of ESLD such as ascites, variceal hemorrhage, hepatic encephalopathy, and renal impairment primarily account for these deaths. Patients with ESLD require increasingly complex medical support and manifest a spectrum of complications and symptoms that have significant impact on both survival and quality of life.

Compromise of the blood supply from microvascular disease, often in association with lack of sensation because of neuropathy, predisposes persons with diabetes mellitus to foot infections. These infections span the spectrum from simple, superficial cellulitis to chronic osteomyelitis. Diabetic foot infections typically take one of the following forms: Cellulitis Deep-skin and soft-tissue infections Acute osteomyelitis Chronic osteomyelitis Cellulitis Tender, erythematous, nonraised skin lesions are present, sometimes with lymphangitis Lymphangitis suggests group A streptococcal infection Bullae are typical of Staphylococcus aureus infection, but occasionally occur with group A streptococci
Describe pre-procedure considerations for administering a subcutaneous injection.
Describe and demonstrate the preparation for administering a subcutaneous injection.
Describe and demonstrate needle and blood safety.
Describe and demonstrate suitable injection sites for subcutaneous injections.
Discuss the appropriate needle and syringe sizes for subcutaneous injection.
Describe and demonstrate the preparation of the substance to be injected.
Describe and demonstrate safe and correct administration of a subcutaneous injection.
Understand and apply Occupational Safety and Health Administration (OSHA) guidelines.
Understand and apply drug administration safety guidelines (seven rights).
Understand correct post-procedure considerations.
Describe and demonstrate correct documentation.
Define and demonstrate correct recording and reporting procedures.
Define and use related medical terminology.
Explain the Patient Privacy Rule (HIPAA), Patient Safety Act, and Patients' Bill of Rights.
www.simtics.com

His father, Dr. Joseph Dello Russo, helped turn Lasik eye surgery into the widespread procedure it is today. Now he explains a new technique and how it differs.
USMLE Step 2 CS - Numbness Weakness Full Video


Folic acid, which is also called folate, is a B vitamin. The best food sources of folic acid are fortified cereals. Folic acid plays an important role in the production of red blood cells and helps your baby's neural tube develop into her brain and spinal cord.


Carotid Stenosis and what it means. The detection and treatment of carotid artery disease for the prevention of stroke is one of the most effective treatments in all of medicine.
