- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

A prenatal ultrasound (also called a sonogram) is a noninvasive diagnostic test that uses sound waves to create a visual image of your baby, placenta, and uterus, as well as other pelvic organs. It allows your healthcare practitioner to gather valuable information about the progress of your pregnancy and your baby's health. During the test, an ultrasound technician (sonographer) transmits high-frequency sound waves through your uterus that bounce off your baby. A computer then translates the echoing sounds into video images that reveal your baby's shape, position, and movements. (Ultrasound waves are also used in the handheld instrument called a Doppler that your practitioner uses during your prenatal visits to listen to your baby's heartbeat.) You may have an early ultrasound at your practitioner's office at 6 to 10 weeks to confirm and date the pregnancy. Or you may not have one until the standard midpregnancy ultrasound between 16 and 20 weeks. That's when you may learn your baby's sex, if you like. (The technician will probably present you with a grainy printout of the sonogram as a keepsake.) You may also have a sonogram as part of a genetic test, such as the nuchal translucency test, chorionic villus sampling, or amniocentesis, or at any other time if there are signs of a problem with your baby. You'll have more frequent ultrasounds if you have diabetes, hypertension, or other medical complications.

Dialysis Fistula clip from full video on Dialysis Options

Description: Use warm water and sea salt. Soak the wart for 10 to 15 minutes in warm salt water to moisten the skin. Scrape the dead skin layers off the wart using a nail file, pumice stone or mild sandpaper. You could also use your fingers, but wash them thoroughly before and after, as warts can easily spread.

Home hemodialysis gives you the flexibility to fit treatment into your lifestyle and may help you feel better with fewer medications and dietary restrictions. Watch this video to find out about how home hemodialysis could be right for you, and visit our website to learn more: www.FreseniusKidneyCare.com/HHD. #HomeDialysis #DialysisTreatment #KidneyDialysis
Subscribe to Our YouTube Channel
Subscribe Here: https://www.youtube.com/user/FMSMarketing
Find Fresenius Kidney Care Online at:
Website: https://www.freseniuskidneycare.com/
Facebook:@FreseniusKidneyCare
https://www.facebook.com/FreseniusKidneyCare/
Pinterest: Fresenius Kidney Care
https://www.pinterest.com/FreseniusKidneyCarePins/

Different types of Abscess- Drainage and Aspiration of Pus.

Revision of Mini Gastric ByPass
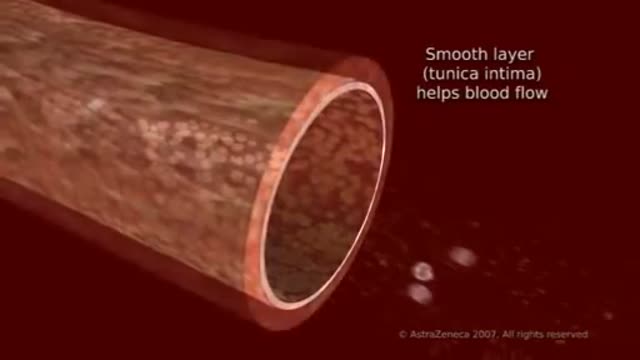
To understand high blood cholesterol (ko-LES-ter-ol), it helps to learn about cholesterol. Cholesterol is a waxy, fat-like substance that’s found in all cells of the body. Your body needs some cholesterol to make hormones, vitamin D, and substances that help you digest foods. Your body makes all the cholesterol it needs. However, cholesterol also is found in some of the foods you eat. Cholesterol travels through your bloodstream in small packages called lipoproteins (lip-o-PRO-teens). These packages are made of fat (lipid) on the inside and proteins on the outside. Two kinds of lipoproteins carry cholesterol throughout your body: low-density lipoproteins (LDL) and high-density lipoproteins (HDL). Having healthy levels of both types of lipoproteins is important. LDL cholesterol sometimes is called “bad” cholesterol. A high LDL level leads to a buildup of cholesterol in your arteries. (Arteries are blood vessels that carry blood from your heart to your body.) HDL cholesterol sometimes is called “good” cholesterol. This is because it carries cholesterol from other parts of your body back to your liver. Your liver removes the cholesterol from your body.

MotionLit can help you multiply the value of your case by portraying the mechanisms of injuries in a 3D Accident Reconstruction Animation. Call (855)850-0650 or visit motionlit.com to learn & earn more for your client!
MotionLit is a one-stop-shop for litigators, offering complete trial services from video production, animation, litigation support, exhibit design, trial technician, and video depositions. Our visuals have proven to help attorneys obtain record-breaking verdicts with our persuasive trial presentations, settlement documentaries, and demonstratives.
Contact Us At:
www.motionlit.com
(213) 291 9141
info@motionlit.com
Follow Us On:
Twitter: @motionlit
Instagram: https://www.instagram.com/motionlit/
Facebook: https://www.facebook.com/MotionLit/

1 yıldır astım tedavisi gören 45 yaşında bayan hasta. Nefes darlığı şikayeti artması üzerine yapılan bronkoskopide trakea lümenini tamayakın tıkayan kitle gözlendi. Coller insizyonu ve parsiyel sternotomi ile yaklaşıldı ve rezeke edildi.

An ectopic pregnancy results when a fertilized egg implants outside the uterus. Unfortunately, there's no way to transplant an ectopic pregnancy into your uterus, so ending the pregnancy is the only option. About 2 percent of pregnancies are ectopic. Because ectopic pregnancy is potentially dangerous for you, it's important to recognize the early signs and get treatment as soon as possible.

Implant comparison: Coloplast vs AMS for Penile Implants

Rapid cycling is a pattern of frequent, distinct episodes in bipolar disorder. In rapid cycling, a person with the disorder experiences four or more episodes of mania or depression in one year
New device claims to stimulate brain for depression treatment

Central Venous Catheter Placement & Pulmonary Artery Catheter Video

The principal signs of cerebellar dysfunction are the following: Ataxia: unsteadiness or incoordination of limbs, posture, and gait. A disorder of the control of force and timing of movements leading to abnormalities of speed, range, rhythm, starting, and stopping.
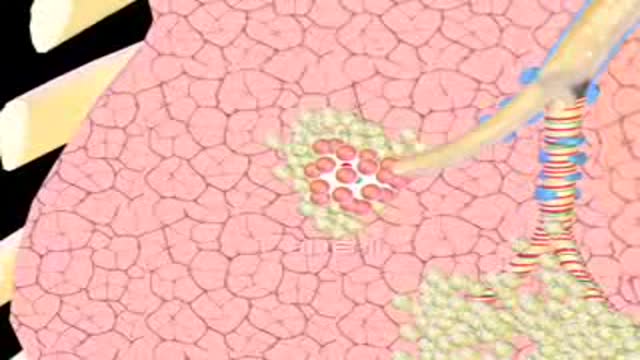
Emphysema gradually damages the air sacs (alveoli) in your lungs, making you progressively more short of breath. Emphysema is one of several diseases known collectively as chronic obstructive pulmonary disease (COPD). Smoking is the leading cause of emphysema. Your lungs' alveoli are clustered like bunches of grapes. In emphysema, the inner walls of the air sacs weaken and eventually rupture — creating one larger air space instead of many small ones. This reduces the surface area of the lungs and, in turn, the amount of oxygen that reaches your bloodstream. When you exhale, the damaged alveoli don't work properly and old air becomes trapped, leaving no room for fresh, oxygen-rich air to enter. Treatment may slow the progression of emphysema, but it can't reverse the damage.
Watch that video to know Increase Male Genital Length Naturally With These 5 Methods

Most healthy children are inattentive, hyperactive or impulsive at one time or another. It’s normal for preschoolers to have short attention spans and be unable to stick with one activity for long. Even in older children and teenagers, attention span often depends on the level of interest. The same is true of hyperactivity. Young children are naturally energetic — they often are still full of energy long after they’ve worn their parents out. In addition, some children just naturally have a higher activity level than others do. Children should never be classified as having ADHD just because they’re different from their friends or siblings. Children who have problems in school but get along well at home or with friends are likely struggling with something other than ADHD. The same is true of children who are hyperactive or inattentive at home, but whose schoolwork and friendships remain unaffected.
Stem-cell therapy is the use of stem cells to treat or prevent a disease or condition. Bone marrow transplant is the most widely used stem-cell therapy, but some therapies derived from umbilical cord blood are also in use...
