- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Central Venous Catheter Placement & Pulmonary Artery Catheter Video
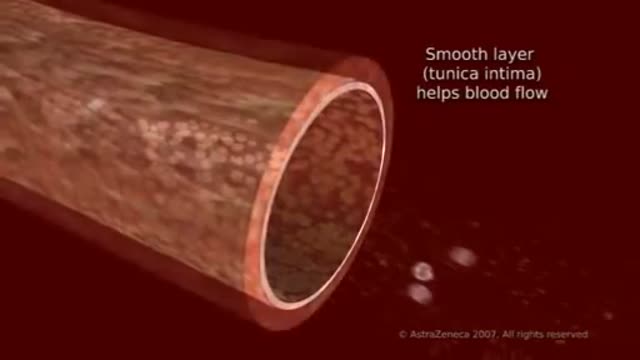
To understand high blood cholesterol (ko-LES-ter-ol), it helps to learn about cholesterol. Cholesterol is a waxy, fat-like substance that’s found in all cells of the body. Your body needs some cholesterol to make hormones, vitamin D, and substances that help you digest foods. Your body makes all the cholesterol it needs. However, cholesterol also is found in some of the foods you eat. Cholesterol travels through your bloodstream in small packages called lipoproteins (lip-o-PRO-teens). These packages are made of fat (lipid) on the inside and proteins on the outside. Two kinds of lipoproteins carry cholesterol throughout your body: low-density lipoproteins (LDL) and high-density lipoproteins (HDL). Having healthy levels of both types of lipoproteins is important. LDL cholesterol sometimes is called “bad” cholesterol. A high LDL level leads to a buildup of cholesterol in your arteries. (Arteries are blood vessels that carry blood from your heart to your body.) HDL cholesterol sometimes is called “good” cholesterol. This is because it carries cholesterol from other parts of your body back to your liver. Your liver removes the cholesterol from your body.

Watch that video to know the Natural Ways to Whiten Teeth at Home

Different types of Abscess- Drainage and Aspiration of Pus.
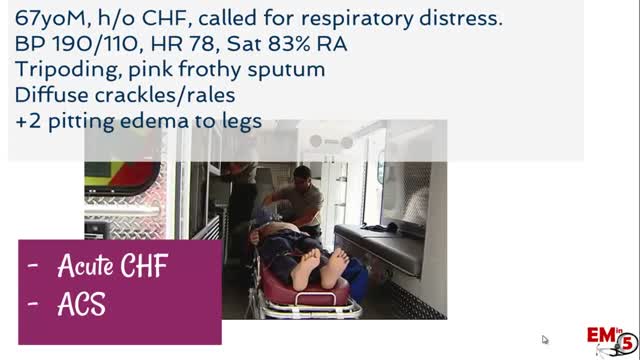
Hypertensive urgency must be distinguished from hypertensive emergency. Urgency is defined as severely elevated blood pressure (ie, systolic >220 mm Hg or diastolic >120 mm Hg) with no evidence of target organ damage.
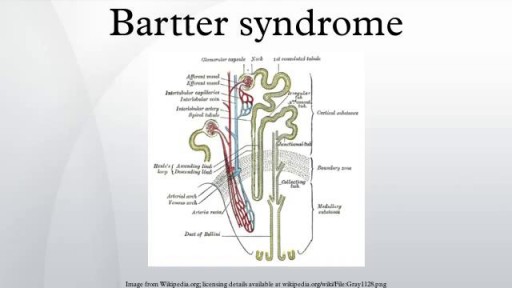
Bartter syndrome is a rare inherited defect in the thick ascending limb of the loop of Henle. It is characterized by low potassium levels (hypokalemia), increased blood pH (alkalosis), and normal to low blood pressure. There are two types of Bartter syndrome: neonatal and classic

An ectopic pregnancy results when a fertilized egg implants outside the uterus. Unfortunately, there's no way to transplant an ectopic pregnancy into your uterus, so ending the pregnancy is the only option. About 2 percent of pregnancies are ectopic. Because ectopic pregnancy is potentially dangerous for you, it's important to recognize the early signs and get treatment as soon as possible.

Dialysis Fistula clip from full video on Dialysis Options

Most healthy children are inattentive, hyperactive or impulsive at one time or another. It’s normal for preschoolers to have short attention spans and be unable to stick with one activity for long. Even in older children and teenagers, attention span often depends on the level of interest. The same is true of hyperactivity. Young children are naturally energetic — they often are still full of energy long after they’ve worn their parents out. In addition, some children just naturally have a higher activity level than others do. Children should never be classified as having ADHD just because they’re different from their friends or siblings. Children who have problems in school but get along well at home or with friends are likely struggling with something other than ADHD. The same is true of children who are hyperactive or inattentive at home, but whose schoolwork and friendships remain unaffected.

Watch that video to know if you have Trypophobia

A check up at the Ear Nose & Throat doctor to make sure Genie's Opera singing vocal chords are working properly.
How a Clot Can Become a Pulmonary Embolism
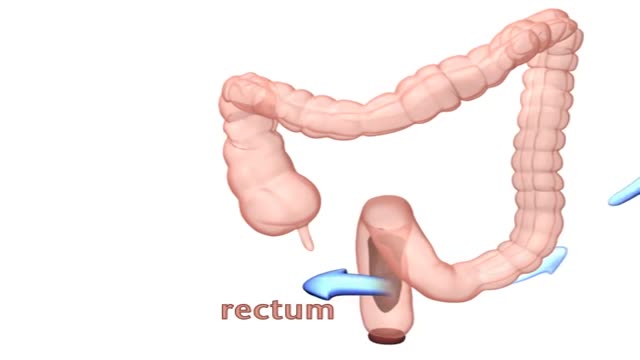
Encopresis is a problem that children age four or older can develop due to chronic (long-term) constipation. With constipation, children have fewer bowel movements than normal, and the bowel movements they do have can be hard, dry, and difficult to pass. The child may avoid using the bathroom to avoid discomfort.

A visual prosthesis, often referred to as a bionic eye, is an experimental visual device intended to restore functional vision in those suffering from partial or total blindness. In 1983 Joao Lobo Antunes, a Portuguese doctor, implanted a bionic eye in a person born blind.

laparoscopic left adrenalectomy in 150kg patient with Cushings
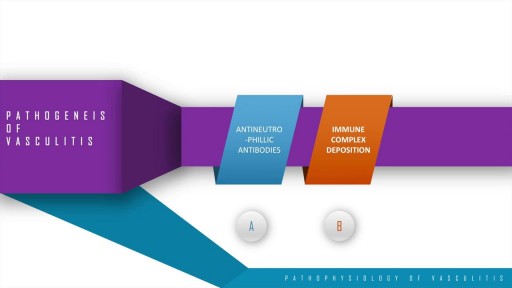
A step wise approach to the pathogenesis, types, disease entities and diagnosis of vasculitis. This discussion also includes the management options of vasculitis and their adverse drug reactions. In essence, vasculitis is a clfinicopathologic process characterised by inflammation and damage of blood vessels. This may be mainly due to three pathological processes which include immune complex deposition, anti-neutrophillic antibody formation and pathological T lymphocyte response and granuloma formation. The disease entities include Wegner's granulomatosis, Churg Strauss and many others. These present with palpable purpura, unexplained renal dysfunction etc which can be diagnosed based on biopsy and angiogram.
A carotid endarterectomy is performed in a sterile surgical suite or standard operating room. You may go home the same day or stay 1–2 nights after the procedure depending on your medical condition. You receive a local anesthetic or general anesthesia. Your vascular surgeon makes an incision at the front of your neck. After removing the plaque from the artery your vascular surgeon repairs the artery by stitching in a natural graft (formed from a piece of vein from elsewhere in your body) or a woven patch. The incision is closed

Don't cleanse your contact lenses with tap water.

Head Eye and ENT Physical Examination
Intrauterine insemination (IUI) is a fertility treatment that involves placing sperm inside a woman's uterus to facilitate fertilization. The goal of IUI is to increase the number of sperm that reach the fallopian tubes and subsequently increase the chance of fertilization.
