- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Genital warts are growths on the skin of the genital area and around the anus. They are caused by certain types of the human papilloma virus (HPV). There are more than 100 types of HPV. Some types of HPV produce warts on different parts of the body, like plantar warts on the feet and common hand warts. There is no specific treatment for HPV, but there are treatments for health problems caused by HPV. Genital warts can be treated by your healthcare provider, or with prescription medication. HPV-related cancers are more treatable when diagnosed and treated promptly. For more information, visit www.cancer.org.

Minimally invasive surgery has been shown to be feasible and safe in pediatric patients since 1975 when laparoscopic surgery was first used to treat a small bowel obstruction. Laparoscopy is an option for surgical repair of inguinal hernias in addition to the traditional open approach.

How to approach histology for Human Anatomy students. Using a key will help get you through it! Add some penguin fairy dust will help too!
Please note: I mis-spoke and said "striated" instead of "stratified epithelium" a couple of times... apologies!
There are lots of histology keys out there, but the one I showed in the video is here: http://www.penguinprof.com/upl....oads/8/4/3/1/8431323
Want more?
Subscribe: http://www.youtube.com/user/ThePenguinProf
FB Page: https://www.facebook.com/ThePenguinProf
Twitter: https://twitter.com/penguinprof
Web: http://www.penguinprof.com/
---------------------------------------------------------------------------------------------------
Details:
Tissue in the human body:
Epithelial: Is made of cells arranged in a continuous sheet with one or more layers, has apical & basal surfaces.
A basement membrane is the attachment between the basal surface of the cell & the underlying connective tissue.
Two types of epithelial tissues: (1) Covering & lining epithelia and (2) Glandular Epithelium.
The number of cell layers & the shape of the cells in the top layer can classify epithelium.
Simple Epithelium - one cell layer
Stratified epithelium - two or more cell layers
Pseudostratified Columnar Epithelium - When cells of an epithelial tissue are all anchored to the basement Membrane but not all cells reach the apical surface.
Glandular Epithelium -- (1) Endocrine: Release hormones directly into the blood stream and (2) Exocrine - Secrete into ducts.
Connective: contains many different cell types including: fibroblasts, macrophages, mast cells, and adipocytes. Connective Tissue Matrix is made of two materials: ground substance - proteins and polysaccharides, fiber -- reticular, collagen and elastic.
Classification of Connective Tissue:
Loose Connective - fibers & many cell types in gelatinous matrix, found in skin, & surrounding blood vessels, nerves, and organs.
Dense Connective - Bundles of parallel collagen fibers& fibroblasts, found in tendons& ligaments.
Cartilage - Cartilage is made of collagen & elastin fibers embedded in a matrix glycoprotein & cells called chondrocytes, which was found in small spaces.
Cartilage has three subtypes:
Hyaline cartilage -- Weakest, most abundant type, Found at end of long bones, & structures like the ear and nose,
Elastic cartilage- maintains shape, branching elastic fibers distinguish it from hyaline and
Fibrous Cartilage - Strongest type, has dense collagen & little matrix, found in pelvis, skull & vertebral discs.
Muscle: is divided into 3 categories, skeletal, cardiac and smooth.
Skeletal Muscle -- voluntary, striated, striations perpendicular to the muscle fibers and it is mainly found attached to bones.
Cardiac Muscle -- involuntary, striated, branched and has intercalated discs
Smooth Muscle -- involuntary, nonstriated, spindle shaped and is found in blood vessels & the GI tract.
Nervous: Consists of only two cell types in the central nervous system (CNS) & peripheral nervous system (PNS):
Neurons - Cells that convert stimuli into electrical impulses to the brain, and Neuroglia -- supportive cells.
Neurons -- are made up of cell body, axon and dendrites. There are 3 types of neurons:
Motor Neuron -- carry impulses from CNS to muscles and glands,
Interneuron - interpret input from sensory neurons and end responses to motor neurons
Sensory Neuron -- receive information from environment and transmit to CNS.
Neuroglia -- is made up of astrocytes, oligodendrocytes, ependymal cells and microglia in the CNS, and schwann cells and satellite cells in the PNS.

Watch that video to know the Symptoms and Causes Of Female Genital Infections

A surgeon creates an arteriovenous fistula by making a connection between an artery (which carries blood away from the heart) and a vein (which carries blood back to the heart). This artificial connection allows the vein to become larger and for the walls of the vein to thicken, a process termed maturation. A mature fistula makes it easier for the vein to be punctured repeatedly for dialysis. Maturation typically takes three to six months to occur, but in rare cases, can take up to a year. This makes advance planning for an arteriovenous fistula important. When a patient is felt to be approximately a year away from requiring dialysis, the patient should be referred for evaluation for possible creation of an arteriovenous fistula.


***SUBSCRIBE WITHIN THE NEXT 28 DAYS FOR A CHANCE TO WIN $1,000!***
Did you know only 20% of our video content is on YouTube? Try out our membership for FREE today! → https://bit.ly/3mWibYe
Try our NCLEX Prep FREE → https://bit.ly/3xYAOkT
Head to https://bit.ly/3mWibYe to get access to the other 80%, along with 800+ study guides, customizable quiz banks with 3,000+ test-prep questions, and answer rationales!
Popular Playlists:
NCLEX Fluid & Electrolytes: https://bit.ly/39BSHXs
Heart Failure (CHF): https://bit.ly/2u5zfDm
Myocardial Infarction (MI): https://bit.ly/3bN9AAk
Addison’s vs. Cushing: https://bit.ly/2STvute
Diabetes Mellitus & DKA vs HHNS: https://bit.ly/37D8nbs
Cardiomyopathy: https://bit.ly/38CwcSg
IV Fluids: Hypertonic, Hypotonic & Isotonic: https://bit.ly/2P45BWx
SIADH vs Diabetes Insipidus: https://bit.ly/2wq6Bhb
Follow us on social media for more EXCLUSIVE content 👋
More Videos: https://bit.ly/37CRttH
Instagram: https://www.instagram.com/simplenursing.com_
TikTok: https://www.tiktok.com/simplenursing
Thank you for the support & for tuning in!
Remember… don’t be scared, BE PREPARED!

What Is A Body Wrap, Body Wraps Do They Work, Detoxifying Body Wrap, Best Body Wraps For Cellulite -- http://do-body-wraps-work.plus101.com -- Slimming body wraps firm, tighten and detoxify the skin as well as giving instant inch loss whilst removing toxins and from the body. Depending on your body type it is easy to lose up to 15 inches in sixty minutes! All you need to do is start your weight loss program, remain motivated and you will achieve your desired appearance and also reduce stretch marks and cellulite. Slimming body wrap helps achieve an inch loss in every session which can last for approximately 3 months provided you maintain a healthy lifestyle and your current weight. As opposed to other type of treatments body wrap don't need a lot of post treatment. A body wraps helps in detoxification of your body both externally and internally. It cleans blocked body tissues letting your body to firm up as well as aid in holding the newly well cut shape by the firmness body wrap. The slimming body wraps help in getting rid of toxins deposits through detoxification of tissues as well as restraining of lymphatic system. When preparing for a body wrap you should not moisturize, and you should drink plenty of water. During the process women are expected to be only in panties and bra or briefs in the case of men. You are then weighed and measured multiple areas of your body. A solution of citrus and amino nutrient is often applied on your skin to open up your pores. You are the comfortably but firmly wrapped in linen and elastic body wraps for at least half an hour. The main benefits of body wraps include detoxification, skin firming, slimming, body contouring, boosting metabolism, relaxation, redefining your skin texture and stimulating your lymphatic system. Typically spa or salon body wraps costs between 0 and 0 depending on your area, but you can make the same at home for pennies on the dollar! Home body wrap recipes are available at http://do-body-wraps-work.plus101.com
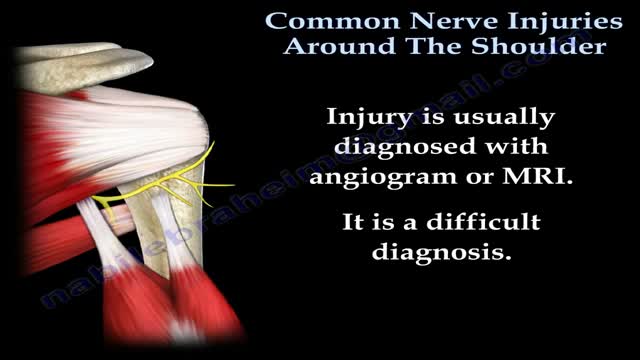
The shoulder and arm receives its nerve supply through the brachial plexus. The brachial plexus is a complex network of nerves which come out of the neck, passes down to the front of the shoulder and then splits into many separate nerves to travel to different muscles and parts of the skin. Normally an arm movement is produced by initially thinking of the movement, then a message passes from the brain, down through the spinal cord to the appropriate nerve. Then the instruction to move is conveyed along the nerve to the specific arm muscle which then contracts and moves the arm.

Psychological testing refers to the administration of psychological tests. A psychological test is "an objective and standardized measure of a sample of behavior" (p. 4). The term sample of behavior refers to an individual's performance on tasks that have usually been prescribed beforehand.

A hernia occurs when an organ or fatty tissue squeezes through a weak spot in a surrounding muscle or connective tissue called fascia. The most common types of hernia are inguinal (inner groin), incisional (resulting from an incision), femoral (outer groin), umbilical (belly button), and hiatal (upper stomach).

This video demonstrates a boatload of excellent teaching points on how to perform a peritoneal tap to remove ascites fluid from the peritoneum.

Septoplasty (SEP-toe-plas-tee) is a surgical procedure to correct a deviated septum — a displacement of the bone and cartilage that divides your two nostrils. During septoplasty, your nasal septum is straightened and repositioned in the middle of your nose.
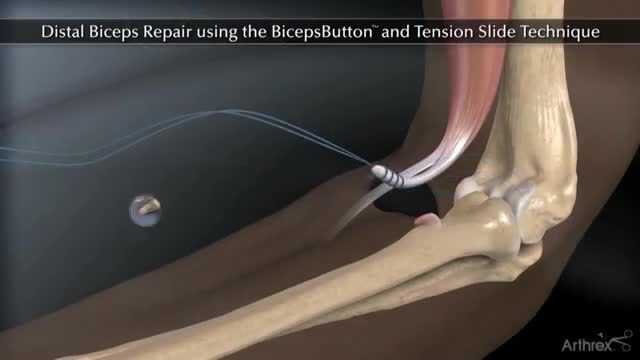
An example of a technique I use in my surgical practice

This 3D medical animation provides a general overview of asthma, the clinical condition of the upper respiratory airways.

By 5 weeks' gestational age, the wolffian (ie, mesonephric) and the müllerian (ie, paramesonephric) ducts have formed from intermediate mesoderm. In the absence of testosterone and müllerian inhibitory substance, the mesonephric ducts regress and the paramesonephric ducts continue to form the female reproductive structures with fusion of the distal portions of the paramesonephric ducts to give rise to the uterine fundus, the cervix, and the upper vagina. These developmental changes are genetically controlled in large part by a series of complex transcriptional signaling pathways including Wnt signaling, Hox genes, and many others. In a female fetus, the wolffian duct disappears except for nonfunctional vestiges. The müllerian duct is lined by a columnar epithelium. This includes the entire cervix and upper vagina to the vaginal plate (ie, sinovaginal bulb). Through a process of squamous metaplasia, the vagina and a variable portion of the ectocervix become covered with squamous epithelium. This process is complete by the fifth month of pregnancy.
kin grafting is a type of graft surgery involving the transplantation of skin. The transplanted tissue is called a skin graft. Skin grafting is often used to treat: Extensive wounding or trauma Burns Areas of extensive skin loss due to infection such as necrotizing fasciitis or purpura fulminans[2] Specific surgeries that may require skin grafts for healing to occur - most commonly removal of skin cancers Skin grafts are often employed after serious injuries when some of the body's skin is damaged. Surgical removal (excision or debridement) of the damaged skin is followed by skin grafting. The grafting serves two purposes: reduce the course of treatment needed (and time in the hospital), and improve the function and appearance of the area of the body which receives the skin graft.

Hemophilia B is a hereditary bleeding disorder caused by a lack of blood clotting factor IX. Without enough factor IX, the blood cannot clot properly to control bleeding.

Fetal heart sound by sonique
A brief screening examination should be conducted checking the face, eyes, mouth, chest, abdomen, spine and limbs to exclude major abnormalities. A strong cry and a widespread pink blush over the face and body are good signs that all is well. Some children may be born with ambiguous genitalia. Ambiguous genitalia is a medical emergency and requires urgent assessment by a paediatrician. If you have sufficient clinical experience, an orogastric tube should be passed when the neonate's mother has suffered polyhydramnios. This excludes oesophageal atresia.
