- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Thumb Tip Regeneration! IV3000 Wound Dressing for Thumb / Finger Trauma

Retro-sigmoid craniotomy (often called "keyhole" craniotomy) is a minimally-invasive surgical procedure performed to remove brain tumors. This procedure allows for the removal of skull base tumors through a small incision behind the ear, providing access to the cerebellum and brainstem. Neurosurgeons may use this approach to reach certain tumors, such as meningiomas and acoustic neuromas (vestibular schwannomas).

What is this white substance coming out from my skin pores everytime I squeeze my nose or chin?
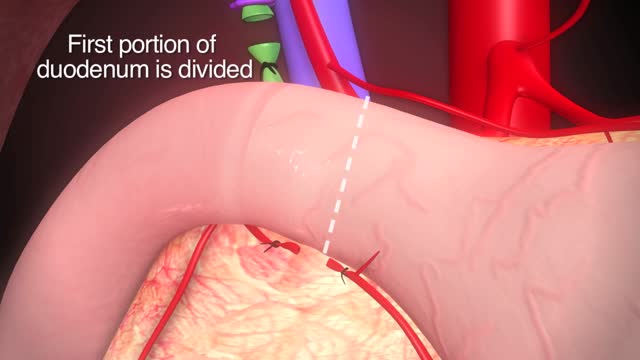
TPIAT is a procedure that lets surgeons remove the pancreas, take out islet cells, and put those islet cells into the liver.

Hemorrhoidectomy Operation Video

A video showing how to catheter the male urethra

The first operation is harvesting the heart from the donor. The donor is usually an unfortunate person who has suffered irreversible brain injury, called "brain death". Very often these are patients who have had major trauma to the head, for example, in an automobile accident. The victim's organs, other than the brain, are working well with the help of medications and other "life support" that may include a respirator or other devices. A team of physicians, nurses, and technicians goes to the hospital of the donor to remove donated organs once brain death of the donor has been determined. The removed organs are transported on ice to keep them alive until they can be implanted. For the heart, this is optimally less than six hours. So, the organs are often flown by airplane or helicopter to the recipient's hospital.

How to remove the Intra Uterine Device (IUD)

A hematoma is a collection of blood outside of a blood vessel. There are several types of hematomas and they are often described based on their location. Examples of hematomas include subdural, spinal, under the finger or toenail bed (subungual), ear, and liver (hepatic). Some causes of hematomas are as pelvic bone fractures, fingernail injuries (subungual), bumps, passing blood clots, blood clot in the leg (DVT), blood cancers, and excessive alcohol use. Symptoms of hematomas depend upon their location and whether adjacent structures are affected by the inflammation and swelling associated with the bleeding and may include

a video discussing the tattoo removal using LASRER
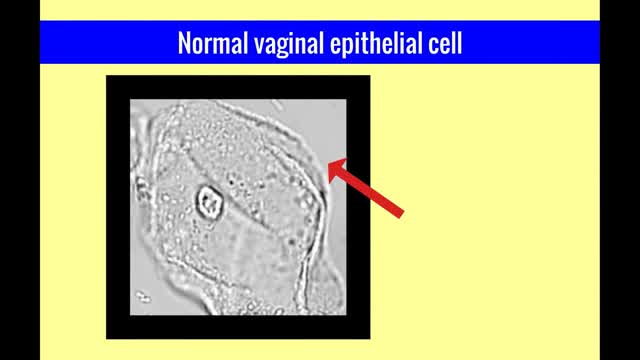
The vulvar vaginal diseases service sees referrals to help women with short--and long--term problems of the outer genital area (vulva), vagina and pelvic floor muscles including: Vulvar vaginal burning, itching, irritation and pain Vulvar Vestibulitis Pain with intercourse Discharge Yeast infections Bacterial vaginosis Pelvic floor muscle dysfunction A patient must be referred by her local health care provider. Services include: Skin care education Examinations-Your healthcare provider will examine you and talk with you about recommendations for treatment and/or management of your symptoms. Some vulvar diseases require a biopsy to diagnose the condition. Referrals-Your healthcare team may refer you to other specialists, including physical therapists or health psychologists. Separate insurance authorization is necessary for these services. The clinic staff provides general education and support to help women cope with these very personal health problems. Following a clinic visit, a letter is promptly sent to your local health care provider. The letter provides the results of your exam and the plan of care.

Craft man’s new ear from rib cartilage and the skin on his forearm
Fremale to male gender reassignment surgery
Everything You Need To Know about injections

In most people, post-concussion syndrome symptoms occur within the first seven to 10 days and go away within three months, though they can persist for a year or more. Post-concussion syndrome treatments are aimed at easing specific symptoms.

This video is really sad. You can literally watch this man dying. He was shot in the chest and rushed to the emergency room. His heart has stopped beating or has arrested. As a last resort, surgeons did an extreme procedure called an open thoracotomy which is that crazy tool you see there that basically splits the ribs open and allows easy open access to the heart. They did this so they could give him a cardiac massage. A cardiac massage is when surgeons are manually trying to pump the heart after it has stopped working on its own (cardiac arrest). Unfortunately he lost so much blood from his gun shot wound and he was pronounced dead. There are cases of patients surviving after having this kind of invasive resuscitation but it is rare.

This video: Polycystic ovary syndrome (PCOS) is a common endocrine system disorder among women of reproductive age. Women with PCOS may have enlarged ovaries that contain small collections of fluid — called follicles — located in each ovary as seen during an ultrasound exam. Infrequent or prolonged menstrual periods, excess hair growth, acne, and obesity can all occur in women with polycystic ovary syndrome. In adolescents, infrequent or absent menstruation may raise suspicion for the condition. The exact cause of polycystic ovary syndrome is unknown. Early diagnosis and treatment along with weight loss may reduce the risk of long-term complications, such as type 2 diabetes and heart disease.

In this video, we will cover the function of the liver and how cancer may arise.

Total Hip Replacement Animation
