- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
ost of us come across this particular sign quite often. Of course, you can just jump to the numerous investigations and one after another, rule out the possible causes, finally getting to the diagnosis. For me, that’s no fun at all. Although I still don’t know whether I am going to become a surgeon or not (embarassing for me, since I’m going to be done with med-school this year), its pretty fascinating. If I were to work in a country whether investigations aren’t that expensive, I would definitely just perform a small examination and take a short history, sending off my patient to get a myriad of investigations, reporting to me after a while, with the diagnosis in his reports.

A walk through of an interactive about male to female sex reassignment surgery.

Dr. Alex Campbell and Dr. Carolina Restrepo of Premium Care Plastic Surgery in Cartagena, Colombia perform a Mommy Makeover on an international patient. Watch the procedure as Dr. Campbell and Dr. Restrepo work together to offer this patient more surgery in less time, which leads to a quicker recovery and better results.
Watch that Recto vaginal Exam Video

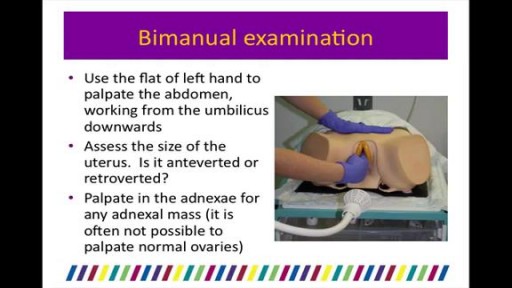
Gynecological Examination

Delivery Video

Parkinson disease (PD) is a common neurodegenerative condition. Typically beginning in the sixth or seventh decade of life, it is characterized by the unilateral onset of resting tremor in combination with varying degrees of rigidity and bradykinesia. PD was originally described by James Parkinson (1755-1824), a man of many talents and interests. Parkinson published works on chemistry, paleontology, and other diverse topics. Early in his career he was a social activist championing the rights of the disenfranchised and poor. His efforts in this area were enough to result in his arrest and appearance before the Privy Council in London on at least one occasion. In collaboration with his son, who was a surgeon, he also offered the first description in the English language of a ruptured appendix. His small but famous publication, "Essay on the Shaking Palsy," was published in 1817, seven years before his death. The clinical descriptions of 6 cases was remarkable in part because he never actually examined the people he described. Instead, he had simply observed these people on the streets of London.
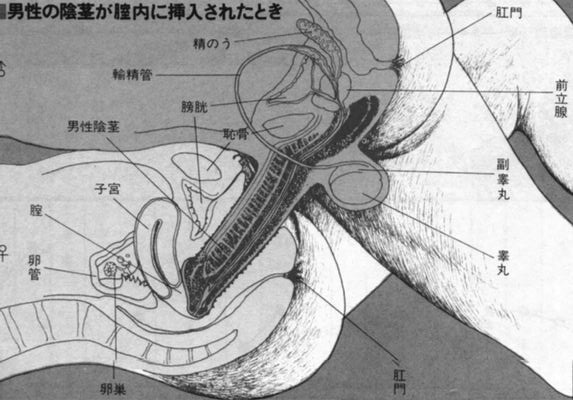
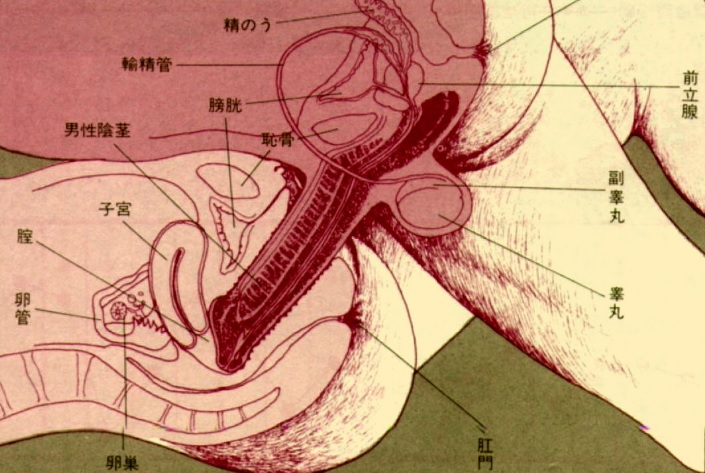
Watch that video to know if it is safe to have anal sex

Frontotemporal degeneration (FTD) is a disease process that results in progressive damage to the temporal and/or frontal lobes of the brain. It causes a group of brain disorders that share many clinical features.
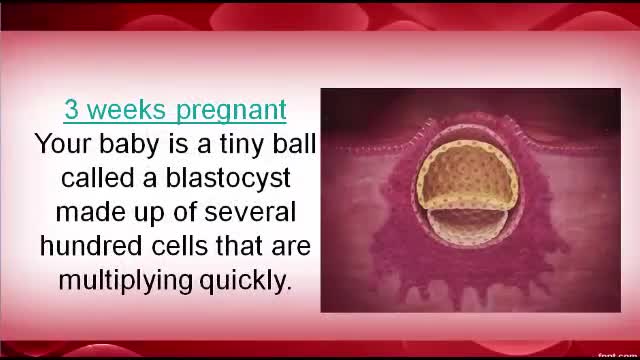
Pregnancy first Trimester


Majority of patients these days prefer PCNL ( Minimal Invasive Telescopic removal of kidney stones broken with lithoclast, removed through a button hole incision ). This patient with a big stone in the pelvis of the kidney wanted it open only so I did an open pyelolithotomy for this patient after a long time as I use to do it in routine in the past. Except for the long incision and scar as compared to PCNL the recovery time was the same and patient went home third day happily walking and eating.
First stage of labour with its signs and symptoms like uterine contractions and the show

Although the Apgar score was developed in 1952 by an anesthesiologist named Virginia Apgar, you also might hear it referred to as an acronym for: Appearance, Pulse, Grimace, Activity, and Respiration. The Apgar test is usually given to a baby twice: once at 1 minute after birth, and again at 5 minutes after birth.

Watch that video of Stuck Sex Toy Medical Removal Surgery

#tummytucksurgery #tummytuckcost #tummytuckresult #drprashantyadav #dezireclinicindia #cosmeticsurgery #plasticsurgery #weightloss #tummytuck #abdominoplasty
Tummy tuck surgery | Weight Loss
Tummy Tuck Marking before surgery
Tummy Tuck Surgery , Tummy Tuck Surgery Cost, Weight Loss with Tummy tuck surgery, tummy tuck surgery result , tummy tuck cost, Abdominoplasty
📞 Delhi - +91 8956880644 | Pune - +91 9222122122 | Bangalore- 8971224700 | Gurugram - 9272007896 | Ahmedabad - 9711162746
Subscribe to our Channel https://www.youtube.com/dezireclinic
💸Cost: call for free consultation | Zero % interest finance options
Subscribe on YouTube : https://youtube.com/dezireplas....ticsurgerycenter?sub
Subscribe on YouTube https://youtube.com/dezireclin....ic?sub_confirmation=
📸 https://www.instagram.com/drprashantdezireclinic/
🌐 http://dezireclinic.in/
Facebook: https://www.facebook.com/drprashantmch/
Twitter: https://twitter.com/drprashantmch
Email: dezireclinicindia@gmail.com
WHY choose Dezire plastic surgery center?
We are leading cosmetic surgery centre in India leading by Dr Prashant Yadav . See hundreds of various cosmetic surgery and real feedback videos. Watch live surgery to gain confidence before deciding surgery
Dr. Prashant Yadav
M.S., M.Ch. (Plastic & Cosmetic Surgery)
#plasticsurgery #cosmeticsurgery #dezireclinicindia #drprashantyadav #dezireplasticsurgerycenter
Watch that video to learn How To Insert Enema
Watch that video to know How To Increase Your Testosterone Levels, Naturally

Alexandra J. Golby, MD, Director, Image-guided Neurosurgery at Brigham and Women’s Hospital, discusses technological advancements to improve the precision of surgery to remove brain tumors.
It’s estimated that each year nearly 80,000 people are diagnosed with primary brain tumors and 100,000 with metastatic brain tumors. Nearly everybody is at risk for developing a brain tumor. Brain tumors can affect people from childhood to the last years of their lives. Men are slightly more affected than women and the causes of most brain tumors are not known.
There are a number of unique challenges in treating brain tumors. One challenge is that primary tumors can have indistinct margins that are difficult to see. Another challenge is that the tissue around a brain tumor is uniquely important and may impact things like language, visual and motor function.
The AMIGO Suite, opened in 2011 at Brigham and Women’s Hospital, is the Advanced Multimodality Image Guided Operating Suite. It's an NIH-funded national center which was developed with the goal of translating technological advances into improvements in surgical and interventional care for patients. In the AMIGO Suite, there is an intraoperative MRI scanner which can be brought in and out of the operating room during surgery to help surgeons visualize a patient’s tumor better.
Image-guided surgery uses the information obtained from advanced imaging and translates that into the planning and execution of surgery by acquiring high resolution and specialty structural images of the brain and also functional images of the brain. These images can be registered to one another and then to the patient's head during surgery. This allows surgeons to pinpoint the location of the tumor as well as the areas that we would like to preserve, areas that serve critical brain functions are located.
One of the big challenges, even with image-guided surgery, is that as we perform the surgery, the configuration of the brain is changing, and we call that brain shift. And it's due to changes in the brain itself and also as we remove tissue, things are constantly shifting and moving. When we're talking about doing brain tumor surgery, a few millimeters of movement can be a big difference. How to measure and track brain shift is an important area of research and a number of technologies are being studied to understand how to measure brain shift during surgery.
The development of various intraoperative imaging technologies allows surgeons to provide the most accurate surgical treatment for each individual patient.
Learn more about precision brain surgery at Brigham and Women’s Hospital:
https://www.brighamandwomens.o....rg/neurosurgery/brai

Dr. Joanna Chikwe, explains how patients may feel after heart surgery.
Learn more about the Smidt Heart Institute at Cedars-Sinai at https://ceda.rs/3meIA2A
Learn more about Dr. Joanna Chikwe at https://ceda.rs/3ul6I6t
Connect with us:
https://twitter.com/CedarsSinai
https://www.facebook.com/CedarsSinai
https://www.instagram.com/CedarsSinai
Cedars-Sinai is a leader in providing high-quality healthcare encompassing primary care, specialized medicine and research. Since 1902, Cedars-Sinai has evolved to meet the needs of one of the most diverse regions in the nation, setting standards in quality and innovative patient care, research, teaching and community service. Today, Cedars- Sinai is known for its national leadership in transforming healthcare for the benefit of patients. Cedars-Sinai impacts the future of healthcare by developing new approaches to treatment and educating tomorrow’s health professionals. Additionally, Cedars-Sinai demonstrates a commitment to the community through programs that improve the health of its most vulnerable residents.
