- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Prompted by the hormone prolactin, the alveoli take proteins, sugars, and fat from your blood supply and make breast milk. A network of cells surrounding the alveoli squeeze the glands and push the milk out into the ductules, which lead to a bigger duct.

The MAKOplasty® procedure is an FDA-cleared treatment option for patients who suffer from osteoarthritis damage in the medial (inner) portion of the knee. ... Only the diseased portion of your knee is removed, leaving the healthy bone and tissue surrounding it untouched.

Haemorrhoids is one of the most common problems seen in surgical OPD. Open haemorrhoidectomy has remained the gold standard for a long time with a high post-operative morbidity. The quest for a better understanding of the pathology of haemorrhoids resulted in the evolvement of stapler haemorrhoidopexy. Our aim is to study the efficacy of stapler haemorrhoidopexy with regards to role of immediate post-operative morbidity. A prospective study of 50 patients (n = 50) with the second- and third-degree symptomatic haemorrhoids was done. The mean age of the patients was 44.1 years. Fourteen patients had co-morbid conditions. The average duration of the operation was 29 min. Patients with the second-degree haemorrhoids had higher rate of complication. The complication rate was 32%. Three patients had urinary retention. Two patients had minor bleeding, and one patient experienced transient discharge. The mean analgesic requirement was 2.4 tramadol, 50 mg injections. Ten patients had significant post-operative pain. Average length of hospital stay was 2.7 days. There were no symptomatic recurrences till date.

Polycystic ovary syndrome (PCOS) is a common endocrine system disorder among women of reproductive age. Women with PCOS may have enlarged ovaries that contain small collections of fluid — called follicles — located in each ovary as seen during an ultrasound exam. Infrequent or prolonged menstrual periods, excess hair growth, acne, and obesity can all occur in women with polycystic ovary syndrome. In adolescents, infrequent or absent menstruation may raise suspicion for the condition. The exact cause of polycystic ovary syndrome is unknown. Early diagnosis and treatment along with weight loss may reduce the risk of long-term complications, such as type 2 diabetes and heart disease.

The video will describe features of right upper lobe collapse. Please see my website for disclaimer.


DR.JUE IS SUGAR LAND' S PREMIERE LUMINEERS AND SNAP ON SMILE DENTIST. DR. JUE HAS BEEN FEATURED ON FOX NEWS FOR LUMINEERS! Lumineers . The Den-Mat Corporation has patented a type of porcelain veneer called Lumineer, and we are proud to announce our full certification in Lumineer application. Lumineers work great for fixing gapped teeth, teeth that slope inward, or teeth that are to small. Because there is no drilling, Lumineers are nearly painless to apply.

Mastitis is an infection of the breast tissue that results in breast pain, swelling, warmth and redness. You also might have fever and chills. Mastitis most commonly affects women who are breast-feeding (lactation mastitis), although sometimes this condition can occur in women who aren't breast-feeding. In most cases, lactation mastitis occurs within the first six to 12 weeks after giving birth (postpartum), but it can happen later during breast-feeding. The condition can cause you to feel run down, making it difficult to care for your baby. Sometimes mastitis leads a mother to wean her baby before she intends to, but continuing to breast-feed, even while taking an antibiotic for the mastitis, is better for you and your baby.
Myeloma is a cancer of the plasma cell, a type of white blood cell that is part of the immune system. This animation explains how a plasma cell can become cancerous and turn into a myeloma cell.

USMLE Step 2 CS - Weight loss This is just preview video. To get full access please visit our website : www.usmletutoring.com

A rare view into fertilization, embryo development, and laboratory procedures performed during an IVF cycle. Take an exclusive look inside one of the most advanced, state-of-the-art in vitro fertilization (IVF) laboratories to see how RMA of New York performs IVF and other advanced reproductive technologies using strict identification standards.
Medical and laboratory video footage documents egg retrieval, insemination, embryo development from cleavage stage (day 2-3) to blastocyst stage (day 5-6), intracytoplasmic sperm injection (ICSI), assisted hatching, embryo transfer and embryo cryopreservation.
Reproductive Medicine Associates of New York
www.rmany.com
635 Madison Avenue, 10th floor
New York, New York 10022
Telephone: (212) 756-5777
Facsimile: (212) 756-5770
15 North Broadway, Garden Level - Suite G
White Plains, New York 10601
Telephone: (914) 997-6200
Facsimile: (914) 997-8111
Reproductive Medicine Associates of New York, Long Island
400 Garden City Plaza, Suite 107
Garden City, NY 11530
Telephone: (516) 746-3633
Facsimile: (516) 746-3622
Reproductive Medicine Associates International Mexico, S.C.
Prolongacion Paseo de la Reforma 1232, Oficina 1213
Colonia Lomas de Bezares
Delegacion Miguel Hidalgo
Mexico, Distrito Federal 11910
Telephone: 011-52-55-2167-2515
Fax: 011-52-55-2167-6434
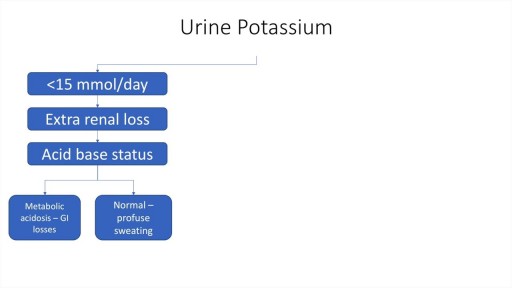
A step by step approach to Hypokalaemia including causes, diagnosis and management.
Watch that video to know How To Remove Teeth Plaque Without Going To The Dentist

During surgery to repair the hernia, the bulging tissue is pushed back in. Your abdominal wall is strengthened and supported with sutures (stitches), and sometimes mesh. This repair can be done with open or laparoscopic surgery. You and your surgeon can discuss which type of surgery is right for you.
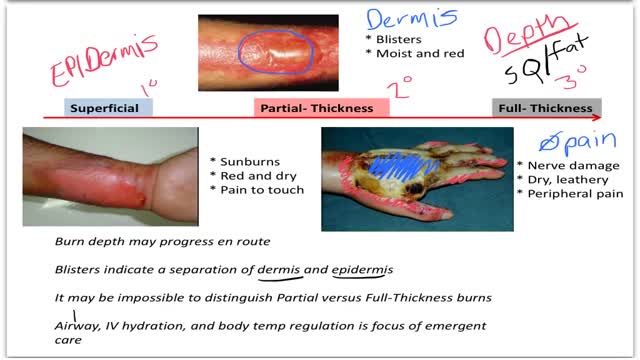
Burns are classified as first-, second-, or third-degree, depending on how deep and severe they penetrate the skin's surface. First-degree burns affect only the epidermis, or outer layer of skin. The burn site is red, painful, dry, and with no blisters. Mild sunburn is an example.
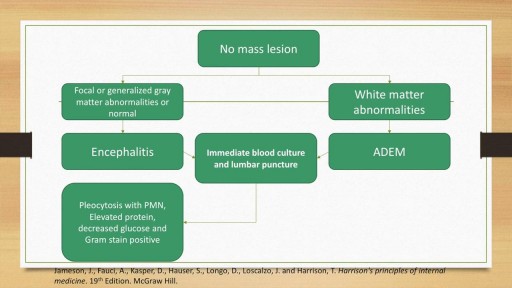
A detailed discussion of the causes, diagnosis and management of the causes of Meningitis and Encephalitis. Includes bacterial, viral, fungal and autoimmune conditions as well as treatment of these conditions. Includes antivirals such as Aciclovir and Ganciclovir as well as IVIG and plasma exchange for autoimmune encephalitis.

Mitosis is the process in which a eukaryotic cell nucleus splits in two, followed by division of the parent cell into two daughter cells. The word "mitosis" means "threads," and it refers to the threadlike appearance of chromosomes as the cell prepares to divide.
Multiple sclerosis (MS) affects the brain and spinal cord. Early MS symptoms include weakness, tingling, numbness, and blurred vision. Other signs are muscle stiffness, thinking problems, and urinary problems. Treatment can relieve MS symptoms and delay disease progression.

Eye tests are important for the detection of many common eye infections and diseases. Eyes are also an important indicator to detect chronic systemic diseases like Hypertension and Diabetes. Must after maxillofacial trauma to rule out any near and late complications emerging for the eyes. 2. There are two perspectives for examining the eyes : 1. Ophthalmic Perspective – because eyes are prone to many infections, diseases and conditions. 2. Maxillofacial Perspective – because the eyes and the orbit forms an integral component of facial and mid-facial fractures and trauma.

Removing ArterioVenous Malformation in Brain
