- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Craft man’s new ear from rib cartilage and the skin on his forearm

Examination of the eye by an ophthalmoscope from the USMLE collection

Chest examination video

Eczema, or atopic dermatitis, is a rash that primarily occurs in people with asthma or allergies. The rash is often reddish and itchy with a scaly texture. Psoriasis is a common skin condition that can cause a scaly, itchy, red rash to form along the scalp, elbows, and joints.Apr 13, 2016
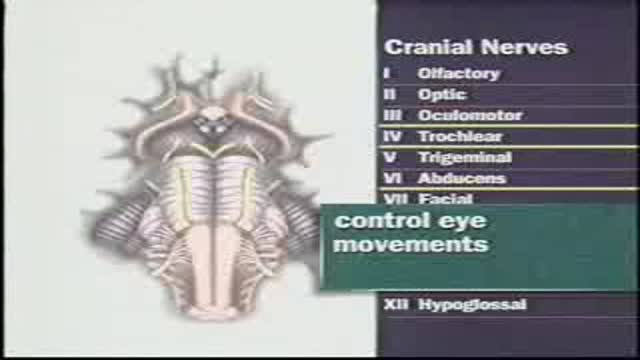
Examination of Cranial nerves III, IV and V: occulomotor,trochlear and trigeminal

Examination of the lymph nodes of the head and the neck and Examination of the thyroid gland
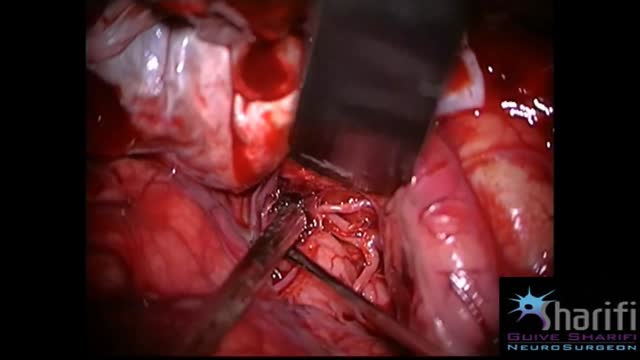
The goal of surgical clipping is to isolate an aneurysm from the normal circulation without blocking off any small perforating arteries nearby. Under general anesthesia, an opening is made in the skull, called a craniotomy. The brain is gently retracted to locate the aneurysm. A small clip is placed across the base, or neck, of the aneurysm to block the normal blood flow from entering. The clip works like a tiny coil-spring clothespin, in which the blades of the clip remain tightly closed until pressure is applied to open the blades. Clips are made of titanium and remain on the artery permanently.

How to Start an IV Like a Pro (Nursing Skills)
Get the full lesson here: https://nursing.com/lesson/ski....lls-02-01-starting-a
FREE Nursing School Cheat Sheets at: http://www.NURSING.com
Welcome to the NURSING Family, we call it the most supportive nursing cohort on the planet.
At NURSING.com, we want to help you remove the stress and overwhelm of nursing school so that you can focus on becoming an amazing nurse.
Check out our freebies and learn more at: (http://www.nursing.com)
In our Nursing Skills course, we show you the most common and most important skills you will use as a nurse! We included everything from bed baths, to inserting a foley, to advanced skills like chest tube management.
How to Start an IV Like a Pro (Nursing Skills):
This video covers the nursing skill of starting an IV. Here are some tips and tricks to hit that vein every time!
Bookmarks:
0:07 Introduction to starting an IV
0:32 First steps/ Locating a good vein
1:03 Preparing supplies
1:59 Tourniquet replacement
2:11 Cleaning the site
2:26 Inspecting the angiocath
2:46 How to insert the angiocath
3:19 Stabilizing the catheter
3:53 Dressing the catheter
4:19 Labeling the dressing
4:25 Sharps and trash disposal
4:34 Closing words of inspiration
Visit us at http://www.nursing.com/medical-inform... for disclaimer information.
NCLEX®, NCLEX-RN® are registered trademarks of the National Council of State Boards of Nursing, INC. and hold no affiliation with NURSING.com.

Watch that video to know if it is safe to have intercourse during her period

A 30 YEAR WOMEN WITH INTRACTABLE BILIARY COLIC
CASE REPORT: This 30 year women developed severe pain right upper quadrant for last 10 days. She sought many consultations and was given intravenous analgesics both (nonnarcortic and narcotic). Pain did not subside and she sought my consultation. Examination revealed her to be in agony with severe upper abdominal pain. General physical examination was otherwise unremarkable. Abdominal examination revealed mild tenderness in right hypochondrium with doubtful Murphy's sign. Urgent abdominal ultrasound showed a linear structure in bile ducts making slow writhing movements. The structure had an anechoic tube (alimentary canal) inside suggestive of a large Ascarid. Urgent ERCP was performed and bile duct and pancreatic duct cannulated selectively. Pancreatic duct was normal. Bile ducts contained a long linear filling defect extending from lower end of common bile duct to right intrahepatic duct (see image gallery for ERCP plate). A basket was introduced in the duct (see video clip) and the linear structure was engaged with soft closure and extracted out of the bile duct. Accompanying the basket was a 25 cm thick highly motile Ascarid. To recover the worm, endoscope was withdrawn along with the basket and the friendly catch. While the endoscope was being withdrawn and the basket was in the duodenum with the worm out of bile duct, patient indicated of relief of abdominal pain. A relook cholangiogram showed no more structures in the duct. She was given antihelmintic therapy and passed hundreds of worms with the feces. The worms recovered form stools were both male and female population and varied in length and size. However the lone worm recovered form bile ducts was the longest and the thickest male worm. The phenomenal behavior of this ubiquitous infection remains unexplained.

NEUROLOGICAL EXAMINATION

Watch that video to know How To Whiten Your Yellow Teeth Naturally at Home
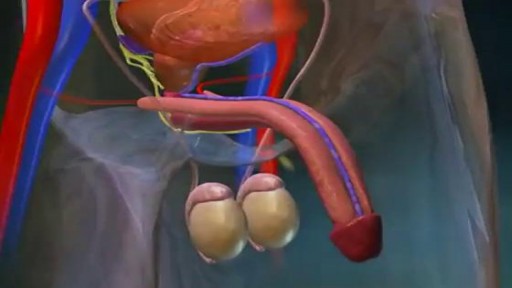
What Happens During an Erection?
In order to attain an erection, messages from the brain and other sense organs trigger the arteries of the penis to dilate. This allows an increased amount of blood to flow into three columns of spongy tissue in the penis.
As the arteries supplying blood to the corpus spongiosum and to the two larger columns, the corpus cavernosa, become filled with blood; the penis grows and becomes rigid. Pressure of the engorged tissue against the veins in the penis effectively traps blood within the penis until climax is reached or the sensation wanes.
What Are Penile Implants?
Impotence, or the inability to attain or maintain an erection, can be caused by a disruption at any stage in this process. Several types of penile implants are available that create an artificial erection. Two common types of implants are the semi-rigid malleable rod and the inflatable implant.
•The semirigid malleable rod is usually made of plastic with a core of flexible wire. These rods can be bent down to conceal the penis under clothing or raised to form an artificial erection.
•The inflatable implant is more complex and involves several working parts: a reservoir of fluid that is implanted into the abdomen, a pump system located in the scrotal sac near the testes, and two inflatable cylinders.
How Penile Implants Help Erectile Fuctioning
In order to attain an erection, the scrotal pump must be squeezed repeatedly to propel fluid into the penile cylinders. When an erection is no longer desired, a release valve is pressed on the side of the pump and the cylinders deflate.
Before Having Penile Implant Surgery
Persons considering these types of implants should speak with their physician or healthcare professional about possible risks and complications.
USMLE Step 2 CS - Numbness Weakness This is just preview video. To get full access please visit our website : www.usmletutoring.com
UCSF Director of Women's Imaging, San Francisco General Hospital, looks at pros and cons of imagining techniques for younger women. Series: "Breast Cancer Prevention and Treatment"
USMLE Step 2 CS - Shoulder Pain This is just preview video. To get full access please visit our website : www.usmletutoring.com
Femoroacetabular impingement (FAI) is a condition in which extra bone grows along one or both of the bones that form the hip joint — giving the bones an irregular shape. Because they do not fit together perfectly, the bones rub against each other during movement. Over time this friction can damage the joint, causing pain and limiting activity.
Carpal tunnel syndrome is a common condition that causes pain, numbness, and tingling in the hand and arm. The condition occurs when one of the major nerves to the hand — the median nerve — is squeezed or compressed as it travels through the wrist. In most patients, carpal tunnel syndrome gets worse over time, so early diagnosis and treatment are important. Early on, symptoms can often be relieved with simple measures like wearing a wrist splint or avoiding certain activities. If pressure on the median nerve continues, however, it can lead to nerve damage and worsening symptoms. To prevent permanent damage, surgery to take pressure off the median nerve may be recommended for some patients.
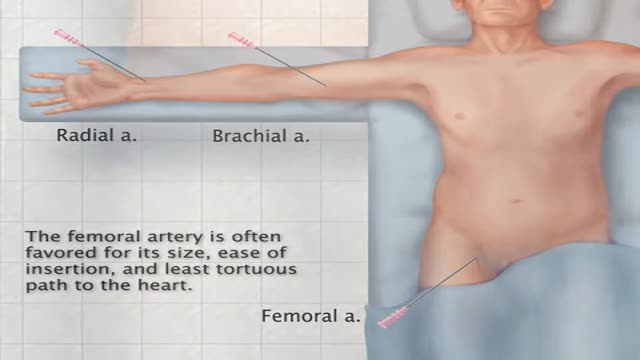
Transfemoral Cardiac Catheterization

You may have heard that some positions, such as your partner on top (missionary position), are better than others for getting pregnant. In fact, there's no evidence to back these theories up. Experts just haven't done the research yet. What experts have done, though, is use scanning to show what's going on inside when you're doing the deed. The research looked at two positions: the missionary position and doggy style. (Doggy style being when you're on all fours, and your partner enters you from behind). Common sense tells us that these positions allow for deep penetration. This means that they're more likely to place sperm right next to your cervix (the opening of your uterus). The scans confirm that the tip of the penis reaches the areas between the cervix and vaginal walls in both of these positions. The missionary position allows the penis to reach the area at the front of the cervix. The rear entry position reaches the area at back of the cervix. It's amazing what some experts spend their time doing, isn't it! Other positions, such as standing up, or woman on top, may be just as good for getting sperm right next to the cervix. We just don't know yet. http://www.babycentre.co.uk/sex-for-getting-pregnant#ixzz4XKnPLbxL
