- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
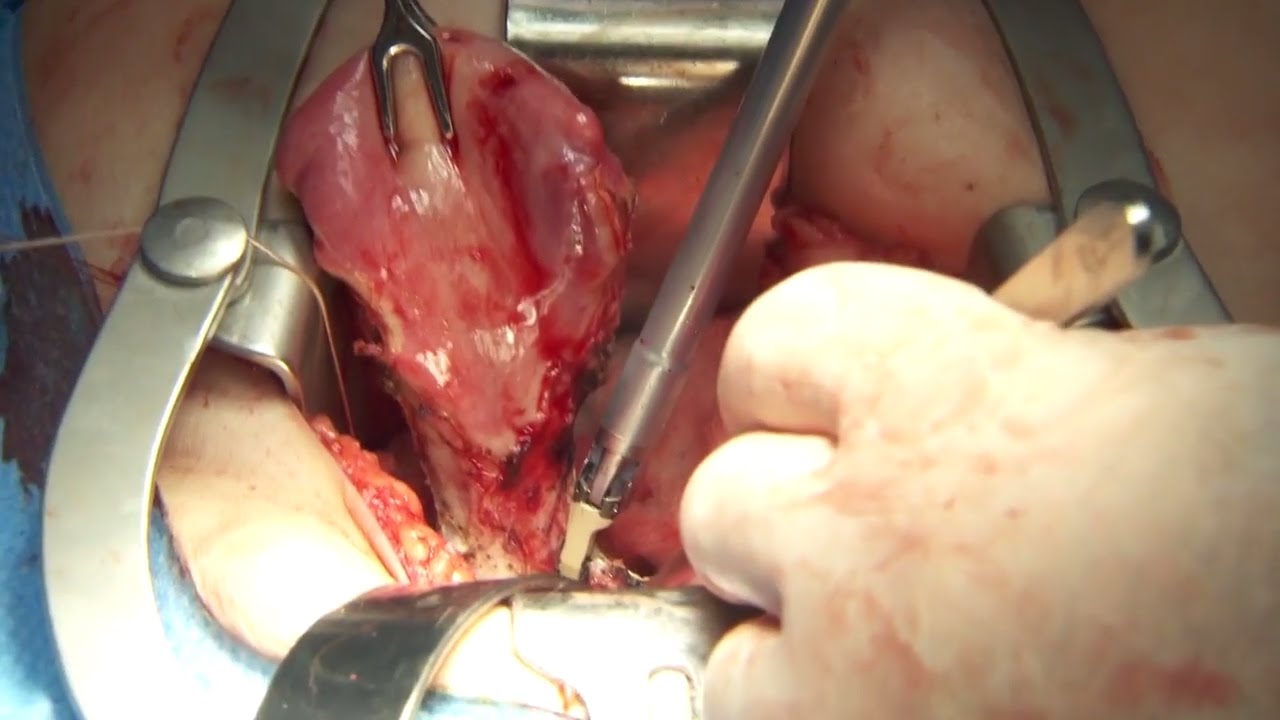
Olympus has extended the value of its award-winning combined surgical energy device, THUNDERBEAT, to open surgical procedures. Watch Dr. Francois Blaudeau master use of THUNDERBEAT Open Extended Jaw (OEJ) in a total abdominal hysterectomy.
http://medical.olympusamerica.com/products/thunderbeat?utm_source=youtube&utm_campaign=Total%20Abdominal%20Hysterectomy%20Surgery%20-%20THUNDERBEAT&utm_medium=description&utm_term=energy&utm_content=surgical

This video is brought to you by the Stanford Medicine 25 to teach you the common causes of shoulder pain and how to diagnose them by the physical exam.
The Stanford Medicine 25 program for bedside medicine at the Stanford School of Medicine aims to promote the culture of bedside medicine to make current and future clinicians and other healthcare provides better at the art of physical diagnosis and more confident at the bedside of their patients.
Visit us:
Website: http://stanfordmedicine25.stanford.edu/
Blog: http://stanfordmedicine25.stanford.edu/blog.html
Facebook: https://www.facebook.com/StanfordMedicine25
Twitter: https://twitter.com/StanfordMed25
Diagnoses covered in this video:
Rotator Cuff Pathology
Impingement Syndrome
Biceps Tendinopathy
Adhesive Capsulitis (Frozen Shoulder)
Acromioclavicular (AC) Joint Disease
Shoulder Instability
Labral Tears (SLAP Lesions)

Human
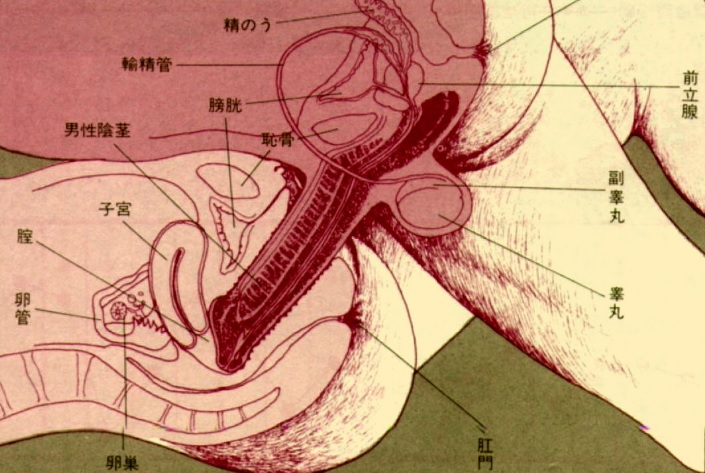
Watch that video to know How To Increase Your Testosterone Levels, Naturally

The Da Vinci Surgical System Robot has benefits for the patient undergoing mitral valve repair and the surgeon performing the procedure. Cardiothoracic Surgeon Thomas Molloy, MD, of St. Joseph Medical Center in Tacoma, WA explains.

A video showing abscess incision and drainage

http://www.landging.com Customize your medical animation | Wow your clients with 3D animation | Outsource to China and reduce risk with a trial project.

Brain cyst Surgery

If you've always wanted six-pack abs, but can't seem to get to the gym - there's now a short-cut for that. Researchers at the University of Miami have developed a new plastic surgery technique called abdominal etching. It can reshape belly fat to make you look like you spend a lot of time at the gym.
READ MORE: https://6abc.cm/2Vv5Tu4
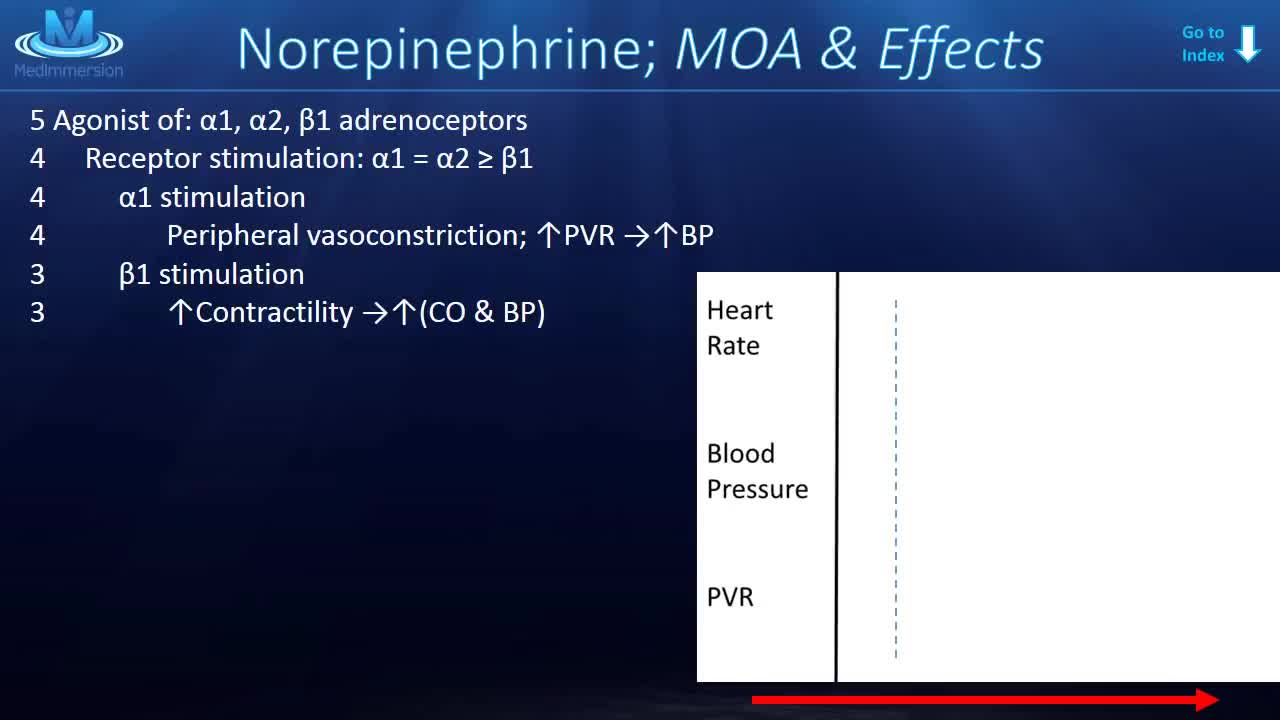
Norepinephrine is synthesized from dopamine by dopamine β-hydroxylase.[7] It is released from the adrenal medulla into the blood as a hormone, and is also a neurotransmitter in the central nervous system and sympathetic nervous system where it is released from noradrenergic neurons.

Paronychia Fingernail Abscess Infection Treatment

In this video, we will cover the function of the liver and how cancer may arise.

Dr. David Salvador provides ultrasonic liposuction for removing fat in West Palm Beach FL.
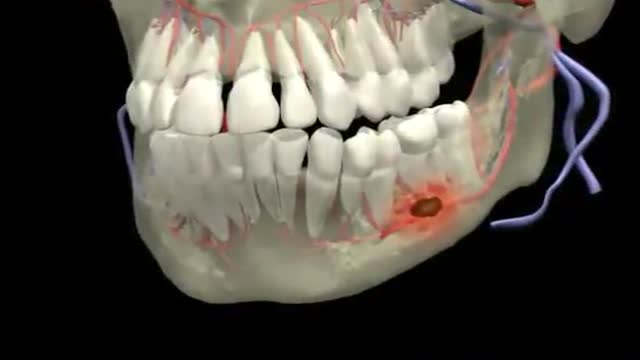
Dental Abscess 3D Animation

Ruth’s testimonial on her amazing experience with cosmetic dental procedures offered by Dr Jamil Alkhoury at Brentwood Family Dental

MEDICAL DESIGN SIALKOT. ®
( Worldwide Medical Health care Supporting Company )
We are the Manufacturer And Exporter Of High
Quality Surgical Instruments, Dental Instruments, Veterinary Instruments, Ophthalmic Instruments, TC Instruments, from Pakistan and are registered member of
SIALKOT CHAMBER OF COMMERCE AND INDUSTRY(SCCI).
We assure our customers Premium Quality Surgical Instruments at very affordable prices, to establish long term mutual Beneficial relationship.
Further we have organized our manufacturing lines in such a way that
our skilled workforce is able to produce specified products as per our
valued customers specification.
MEDICAL DESIGN
Mr. Sajeel Anwar
Address:- Amir Street, Ali Ul haq Road,
Model Town SIALKOT-PAKISTAN
Call : 0092 345 6768889
Email: info@medicaldesignpk.com
Skype : medicaldesignpk

http://barretts-esophagus-cure.info-pro.co Barrett's Esophagus, Barrett's Esophagus Metaplasia, Barrett's Esophagus Bulimia. Are you lost, scared, frustrated, or confused? Have you been recently diagnosed with Barrett’s? Maybe your loved one or a close family member is now a victim of this painful disease. If so, I’d like to share with you some possibly life changing information on how I personally cured my own Barrett’s Esophagus. But before I do I’d like you to take a deep breath, relax for a moment, and let your worry subside because. Even though the Society of Thoracic Surgeons has determined that people with Barrett’s Esophagus are 40x’s more likely to get esophageal cancer, this diagnosis isn’t always a death sentence. Having been a victim of Barrett’s myself, I can relate to the excruciating pain this disease can cause. Maybe you’re like I was, trying to hide the symptoms when the burning, the heartburn, and the PAIN would become so unbearable I’d try doing anything to block it out. I can clearly recall the feeling of those scorching corroding acids inside my throat that would burn like fire, tearing up my esophagus from the inside out. It’s a pain I will NEVER forget. For me, maybe like you, many of my days were spent in anguish and painful agony. Barrett’s Reversed Without Surgery, Pills, PPI Pumps, Antacids, or Drugs. Clicking Here http://barretts-esophagus-cure.info-pro.co

Total Hip Replacement Animation

This patient presented to the ER for umbilical pain and had a history of umbilical hernia. He was concerned about the possibility of incarceration of the hernia.
In this video we explain how the clinical exam helps to differentiate a simple painful hernia from an incarcerated one.
***Thanks to the patient for sharing his history and exam with YouTube world***
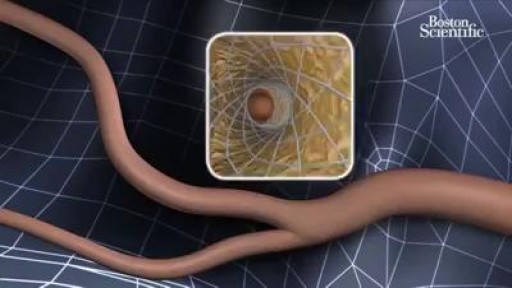
It involves placing a small, expandable tube called a stent in the narrowed artery. This procedure is also called carotid angioplasty and stenting. There are two carotid arteries-one on each side of the neck-that supply blood to the brain. These arteries can be narrowed and damaged by fatty deposits called plaque.
