- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Vital signs help us assess patients in the nursing profession, and there are six common vital signs that we assess as nurses:
1. Heart Rate (Pulse)
2. Respiration Rate
3. Temperature
4. Blood Pressure
5. Pain Rating
6. Oxygen Saturation
This video will demonstrate how to check vital signs (live) on a patient, along with normal rates for each assessment. I also give you a few tips for taking vital signs as a nurse, CNA, or other healthcare profession.
🟣ABG eBook: https://registerednursern.creator-spring.com/
🟣ABG physical book: https://amzn.to/3EsF0Mc (affiliate link)
More nursing skills: https://www.youtube.com/watch?v=G5-Rp-6FMCQ&list=PLQrdx7rRsKfUhd_qQYEbp0Eab3uUKhgKb
Website: https://www.registerednursern.com/
More Videos: https://www.youtube.com/watch?v=R2XMro13dD0&list=UUPyMN8DzkFl2__xnTEiGZ1w
Nursing Gear: https://teespring.com/stores/registerednursern
Instagram: https://www.instagram.com/registerednursern_com/
Facebook: https://www.facebook.com/RegisteredNurseRNs
Twitter: https://twitter.com/NursesRN
Popular Playlists:
NCLEX Reviews: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Fluid & Electrolytes: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing Skills: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf

Misgav Ladach - Joel Cohen approach for breech presentation
How to start a peripheral IV in the dorsum of the hand: clinical nursing skill technique.
Starting an IV (intravenous catheter) can be an intimidating experience for nurses, especially nursing students and new nurses. However, nurses will perform IV insertions often, so this is an important nursing skill to learn.
Before starting an IV, always follow the protocols of your facility, as well as manufacturer's instructions for any supplies used.
In this video, Nurse Sarah demonstrates how to start a peripheral IV in the dorsum of the hand. Prior to inserting the IV, you'll want to do the following:
-Gather supplies
-Perform hand hygiene
-Prepare supplies (including priming the saline flush, removing air from extension tubing, opening packages, completing labels, and any other steps required by your facility.
-Locate a suitable vein
-Perform hand hygiene
-Don gloves
If the patient has a lot of hair, you might want to use clippers to trim the hairs prior to starting the IV. You may also apply a tourniquet to help veins move near the surface of the skin.
Next, you'll want to clean the site using the cleaner that came in the IV start kit, such as ChloraPrep.
Once the site has dried completely, you can insert the IV. Stabilize the vein with your non-dominant hand, and insert the IV's needle into the vein, watching carefully for blood return (or a blood flash) in the chamber. Advance the IV around 2mm more to ensure the plastic cannula is in the vein, then thread the cannula into the vein and press the needle safety button.
Notes: https://www.registerednursern.....com/how-to-start-an-
IV Video Series: https://www.youtube.com/watch?v=MbG_1-_mnoo&list=PLQrdx7rRsKfXr6kruqEpIovf66sxo0gxh
This video also demonstrates how to flush the IV using the push-pause method, how to secure the IV using the Tegaderm dressing that came with the IV start kit, considerations of the different cap types and the clamp sequence, and more.
For more information, watch the complete tutorial.
#nurse #nursing #iv #startiv #ivtherapy
Website: https://www.registerednursern.com/
More Videos: https://www.youtube.com/watch?v=R2XMro13dD0&list=UUPyMN8DzkFl2__xnTEiGZ1w
Nursing Gear: https://teespring.com/stores/registerednursern
Instagram: https://www.instagram.com/registerednursern_com/
Facebook: https://www.facebook.com/RegisteredNurseRNs
Twitter: https://twitter.com/NursesRN
Popular Playlists:
NCLEX Reviews: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Fluid & Electrolytes: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing Skills: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf

Function and Anatomy: The hip is a ball and socket type joint, formed by the articulation of the head of the femur with the pelvis. Normal range of motion includes: abduction 45 degrees, adduction 20-30 degrees, flexion 135 degrees, extension 30 degrees, internal and external rotation. Hip pathology can cause symptoms anywhere around the joint, though frequently pain is anterior and radiates to the groin region. Additionally, pathology outside of the hip can be referred to this region. History and exam obviously help in making these distinctions.

Transurethral resection of the prostate (also known as TURP, plural TURPs and as a transurethral prostatic resection TUPR) is a urological operation. It is used to treat benign prostatic hyperplasia (BPH). As the name indicates, it is performed by visualising the prostate through the urethra and removing tissue by electrocautery or sharp dissection. This is considered the most effective treatment for BPH. This procedure is done with spinal or general anesthetic. A large triple lumen catheter is inserted through the urethra to irrigate and drain the bladder after the surgical procedure is complete. Outcome is considered excellent for 80-90% of BPH patients. Because of bleeding risks associated with the surgery, TURP is not considered safe for many patients with cardiac problems. As with all invasive procedures, the patient should first discuss medications they are taking with their doctor, most especially blood thinners or anticoagulants, such as warfarin (Coumadin), or aspirin. These may need to be discontinued prior to surgery. Postop complications include bleeding (most common), clotting and hyponatremia (due to bladder irrigation).
Additionally, transurethral resection of the prostate is associated with low but important morbidity and mortality.

Mysterious massage from East Asia(CHINA).it can cure cure Erectile dysfunction,can let their life better.This video from mainland of China,so the language is Chinese mandarin.but you can see English show on the video too.Tiedang gong means kongfu of Iron penis&balls.

Watch that Stuck Sex Toy Removal Surgery

http://www.amerra.com In this patient education video from Colorectal Surgical Associates in Houston, Texas, learn more about the single incision laparoscopic colectomy procedure. This minimally invasive procedure uses a mini incision that
results in less pain, fewer complications, earlier recovery, and a smaller scar. Colorectal cancer is the second leading cause of cancer death in the United States. For more information please visit our website: www.csamd.com or call (713)-790-0600.

Suprapubic Catheterization / Cystostomy

In patients age ;::25, HPV DNA testing is the preferred next step in management if the initial cytology shows ASC-US. In this method, samples are collected for both cytology and reflex HPV DNA. If cytology results are positive, HPV DNA testing is performed. If cytology results are negative, the sample for HPV DNA is discarded. HPV DNA testing along with Pap smear at 3 years is recommended if initial cytology shows ASC-US but HPV DNA testing is negative
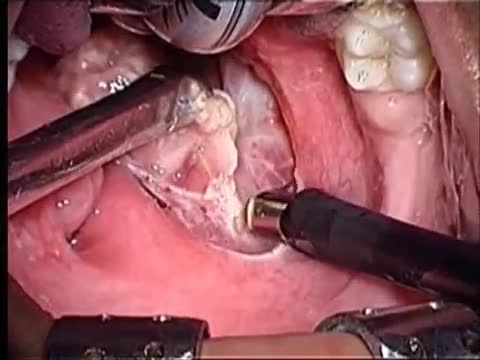
Tonsillectomy (ton-sih-LEK-tuh-me) is the surgical removal of the tonsils, two oval-shaped pads of tissue at the back of the throat — one tonsil on each side. A tonsillectomy was once a common procedure to treat infection and inflammation of the tonsils (tonsillitis). Today, a tonsillectomy is usually performed for sleep-disordered breathing but may still be a treatment when tonsillitis occurs frequently or doesn't respond to other treatments. A tonsillectomy may also be necessary to treat breathing and other problems related to enlarged tonsils and to treat rare diseases of the tonsils.

Today I'm using the best 3D animation to explain WHAT IS DIASTASIS RECTI and what you need to know about diastasis recti after pregnancy! Grab the Complete Diastasis Recti Healing Guide: https://landing.mailerlite.com..../webforms/landing/n0
If you are't sure what video to start with and you just want step-by-step daily instructions you can start my 30-day core healing program. You get a new 10-min core healing video daily for 30 days. https://pregnancyandpostpartum....tv.thinkific.com/cou
How I healed my 4-finger diastasis recti gap:
Jessica Pumple is a registered dietitian, and pre & postnatal fitness instructor and certified pregnancy and postpartum core exercise specialist (CPES). She helps pregnant women stay fit, have healthy babies, and easier labors. She helps new moms with postpartum recovery, to heal and strengthen their core and feel energized after pregnancy!
If you enjoy our content subscribe to our channel, hit the bell button, leave a comment and share with your friends so I can make you more of the videos you enjoy!
Disclaimer: This is general postnatal fitness only. Please check with your doctor or health care provider to see if this video is safe for you. Wait until you get clearance (usually 4-6 weeks or 6-8 weeks after a c-section).You are responsible for your own safety. Don’t do anything that feels unsafe for you or baby. Stop if you have any pain or discomfort, bleeding, chest pain or shortness of breath, dizziness or if you feel unwell. P&P Health Inc., Pregnancy and Postpartum TV and Jessica Pumple are not liable in any way for any injury, loss, damages, costs or expenses suffered by you in relation to this video or its content.
Copyright 2023 P&P Health Inc. All rights reserved
#diastasisrecti #whatisdiastasisrecti #3danimation
Music: Epidemic Sound

A video showing the examination of femoral hernia.
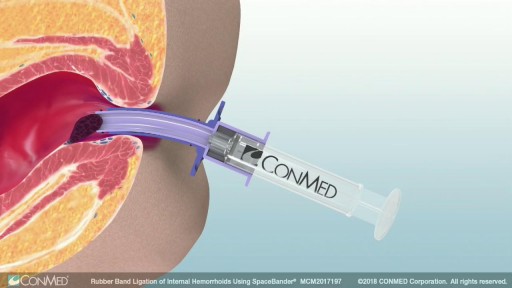
Rubber band ligation is a procedure in which the hemorrhoid is tied off at its base with rubber bands, cutting off the blood flow to the hemorrhoid. This treatment is only for internal hemorrhoids. To do this procedure, a doctor inserts a viewing instrument (anoscope) into the anus. The hemorrhoid is grasped with an instrument, and a device places a rubber band around the base of the hemorrhoid. The hemorrhoid then shrinks and dies and, in about a week, falls off. A scar will form in place of the hemorrhoid, holding nearby veins so they don't bulge into the anal canal. The procedure is done in a doctor's office. You will be asked whether the rubber bands feel too tight. If the bands are extremely painful, a medicine may be injected into the banded hemorrhoids to numb them. After the procedure, you may feel pain and have a sensation of fullness in the lower abdomen. Or you may feel as if you need to have a bowel movement. Treatment is limited to 1 to 2 hemorrhoids at a time if done in the doctor's office. Several hemorrhoids may be treated at one time if the person has general anesthesia. Additional areas may be treated at 4- to 6-week intervals.
Watch that Male Catheter Insertion Procedure
Here's how female-to-male gender reassignment surgery works.

catheterization of the male urethra by a foley catheter
Watch that video of Enema Medical Insertion Procedure


It’s called gamma knife surgery, but there’s no cutting involved.
It’s been used at Mayo Clinic for 30 years as an alternative to open brain surgery.
The patient’s head is held still during the procedure with a headframe, which also serves as a map for the radiation. Using 3D imaging — typically an MRI — as a guide, the gamma knife is targeted directly at the tumor.
And with no hospital stay and minimal side effects, it’s a procedure that is efficient and can be lifesaving.
More health and medical news on the Mayo Clinic News Network. https://newsnetwork.mayoclinic.org/
Journalists: Clean and nat sound versions of this pkg available for download at https://newsnetwork.mayoclinic.org/
Register (free) at https://newsnetwork.mayoclinic.org/request-account/
