- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Watch that video to know How to Treat Premature Ejaculation Naturally
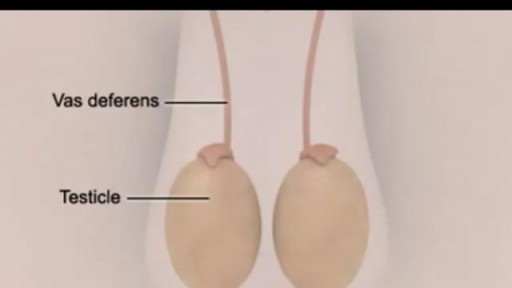
A vasectomy is a simple surgery done by a doctor in an office, hospital, or clinic. The small tubes in your scrotum that carry sperm are cut or blocked off, so sperm can’t leave your body and cause pregnancy. The procedure is very quick, and you can go home the same day. And it’s extremely effective at preventing pregnancy — almost 100%
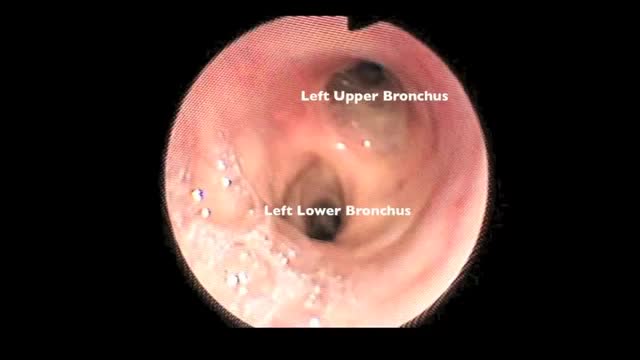
Flexible bronchoscopy is a procedure that allows a clinician to examine the breathing passages (airways) of the lungs (figure 1). Flexible bronchoscopy can be either a diagnostic procedure (to find out more about a possible problem) or a therapeutic procedure (to try to treat an existing problem or condition).

we use a single, tapered PDT dilator and kit . All the equipment and supplies listed must be present at the bed-side, because there is no time to go looking for supplies if an airway emergency occurs during the procedure. Two teams are used simultaneously. One team manages the endo-tracheal tube, and the other manages the placement of the tracheostomy tube
USMLE Step 2 CS - LOC This is just preview video. To get full access please visit our website : www.usmletutoring.com
Histology of Inner Ear 1

During 34 week of pregnancy, the baby is getting ready for delivery, you may feel less wriggling and kicking. Watch out this video to learn more about being 34 weeks pregnant.

A video shoing how to draw blood sample

51 yr old female with right flank pain and recurrent UTI. IVP showed a UPJ calculus on the right.

Dialysis lecture 1. Dialysis Study: EXPERT NOTES for DHA, Bonent, CHT, B.Sc in Dialysis, Diploma in Dialysis https://amzn.eu/d/35Ui1kT
2. Dialysis Study : Q & A: MCQs, Fill in the blanks, True or False https://amzn.eu/d/gGn8u73
1. Dialysis Study :EXPERT NOTES for DHA, Bonent, CHT, B.Sc in Dialysis, Diploma in Dialysis, Naseha Helal.
https://play.google.com/store/....books/details?id=D_7
2. Dialysis Study: Q & A MCQ https://play.google.com/store/....books/details?id=T_3
Whatsapp
https://chat.whatsapp.com/DKCHbgsNwXS1wd7xI31tpr
Telegram
https://t.me/dialysislife PRINCIPLE OF dialysis
https://youtu.be/cfOm0aFmbe8
Dialysis machine alarms
https://youtu.be/-1A1INyDEOg
DDS dialysis disequilibrium syndrome
https://youtu.be/8AqVFiBOkIc
Peritoneal Dialysis
https://youtu.be/iHPPadGmsv0
Itching
https://youtu.be/T83Wm3HHU4M
What is CRRT
https://youtu.be/jPgFnoSEBMU
LVH
https://youtu.be/ZhFL3Z6LHeA
Sorbent dialysis
https://youtu.be/-rie5dC_FkY
RO Water
https://youtu.be/3jlEsK4Lg_I
Carbon filter RO water
https://youtu.be/mJrgtjNafQw
Hemoperfusion
https://youtu.be/UkbBm8rm9Ww
AV fistula or Dialysis fistula
https://youtu.be/uDbyfqCkCbo
Dialysis MCQ
https://youtu.be/zmOj0BL6jVY
AVF cannulation
https://youtu.be/PyqMcHA07zY
Complications of AV fistula
https://youtu.be/a_CXIvuOO_s
Blood clotting during Dialysis
https://youtu.be/9hYNepiO2o8
Muscle crapms
https://youtu.be/09s07Eiqr2k
Hepatitis C
https://youtu.be/qdNj_GhmnSE
Dialysis procedure
https://youtu.be/u1mGqXO5pzQ
Hypotension
https://youtu.be/4EVPmWTSyN8
Heparin free dialysis
https://youtu.be/rFqAn7HcWwM
Plasmapheresis
https://youtu.be/kbgsjjs9krg
Isolated ultrafiltration
https://youtu.be/xp5I5--uWb0
High flux dialyzer
https://youtu.be/gCNsErn1HHM
Urea and Creatinine
https://youtu.be/Id9AIySMQ6c
Practical RO water demo
https://youtu.be/2pXKGMDNS84
Sodium profiling
https://youtu.be/bE_DcBXNB5g
Peritoneal Dialysis
https://youtu.be/vtK6VZsi8AY
Air embolism
https://youtu.be/WJE-xqnQfd8
Dialysate
https://youtu.be/z_nb43bcWsM
How to stop Bleed from fistula
https://youtu.be/N_inLKPhPUc
Dialysis short form
https://youtu.be/3BqB-gODb5o
Dialyzer reprocessing
https://youtu.be/XelfkKsndlc
Dialysis catheter
https://youtu.be/V7y90m4xlv8
How to set KT/V
https://youtu.be/hWXjU8VTQdk
Mircera injection
https://youtu.be/STtd3I3EijA
Dialysis procedure
https://youtu.be/MIdhIgcKRZ8
Dialysis in snake bite poison
https://youtu.be/niA9RI38jyY
Uf profiling
https://youtu.be/wyjpFjD5Hi0
Heparin dose
https://youtu.be/kB56MkzHIQ0
Hyperkalemia
https://youtu.be/1rWWNlcAuio
Change bandages of leaking fistula
https://youtu.be/_0cebWWdjM8
AvF needle
https://youtu.be/GvUxbXxftTk
Polycystic kidney disease
https://youtu.be/IhsMbHFXZG8
Nephrotic syndrome
https://youtu.be/FEEOsIrXxV8
Diabetic nephropathy
https://youtu.be/v-FBIQ7MA4k
Hemodialysis permanent access
https://youtu.be/_YrwxwiR0f8
Sex and dialysis
https://youtu.be/vvl8UT8lK4k
Albumin and dialysis
https://youtu.be/yzG7yD45Nwg
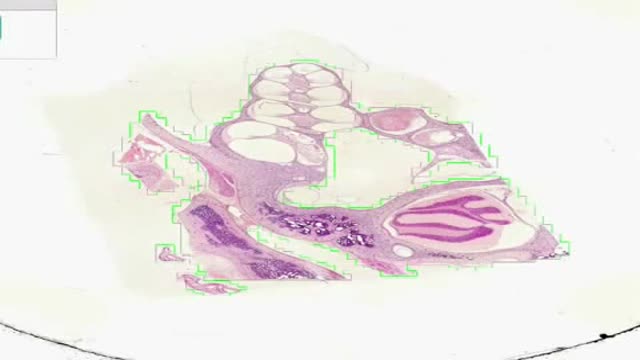
PARAPHARYNGEAL SPACE TUMORS: SURGICAL APPROACH

Shaken baby syndrome symptoms and signs include: Extreme irritability Difficulty staying awake Breathing problems Poor eating Tremors Vomiting Pale or bluish skin Seizures Paralysis Coma Other injuries that may not be initially noticeable include bleeding in the brain and eye, damage to the spinal cord and neck and fractures of the ribs, skull and bones. Evidence of prior child abuse also is common.

A Bone scan or bone scintigraphy is a nuclear scanning test to find certain abnormalities in bone which are triggering the bone's attempts to heal. It is primarily used to help diagnose a number of conditions relating to bones, including: cancer of the bone or cancers that have spread (metastasized) to the bone, locating some sources of bone inflammation (e.g. bone pain such as lower back pain due to a fracture), the diagnosis of fractures that may not be visible in traditional X-ray images, and the detection of damage to bones due to certain infections and other problems.
Nuclear medicine bone scans are one of a number of methods of bone imaging, all of which are used to visually detect bone abnormalities. Such imaging studies include magnetic resonance imaging (MRI), X-ray computed tomography (CT) and in the case of 'bone scans' nuclear medicine. However, a nuclear bone scan is a functional test, which means it measures an aspect of bone metabolism, which most other imaging techniques cannot. The nuclear bone scan competes with the FDG-PET scan in seeing abnormal metabolism in bones, but it is considerably less expensive.
Nuclear bone scans are not to be confused with the completely different test often termed a "bone density scan," DEXA or DXA, which is a low exposure X-ray test measuring bone density to look for osteoporosis and other diseases where bones lose mass, without any bone re-building activity. The nuclear medicine scan technique is sensitive to areas of unusual bone re-building activity because the radiopharmaceutical is taken up by osteoblast cells which build bone. The technique therefore is sensitive to fractures and bone reaction to infections and bone tumors, including tumor metastases to bones, because all these pathologies trigger bone osteoblast activity. The bone scan is not sensitive to osteoporosis or multiple myeloma in bones, and therefore other techniques must be used to assess bone abnormalities from these diseases.

Anatomy of The Upper Limb Joints

Yannas had been studying collagen, a protein found in human skin. Teaming up during the 1970s, the two made a polymer (a chemical compound made of multiple repeating units). Using collagen fibers and a long sugar molecule, they formed a porous (full of small holes) material resembling skin.
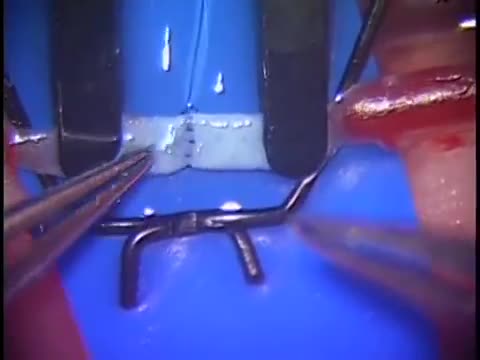
Simple microinstruments and a medical school laboratory microscope were used for anastomosis training. Chicken blood vessels were used as a material for this study. A long segment of blood vessel from the proximal brachial artery to the distal radial artery was used for training. End-to-side anastomosis was practiced first, and the training continued with end-to-end anastomosis of the appropriate segments.

Chickenpox (varicella) is a viral infection that causes an itchy rash with small, fluid-filled blisters. Chickenpox is highly contagious to people who haven't had the disease or been vaccinated against it. Before routine chickenpox vaccination, virtually all people had been infected by the time they reached adulthood, sometimes with serious complications. Today, the number of cases and hospitalizations is down dramatically. For most people, chickenpox is a mild disease. Still, it's better to get vaccinated. The chickenpox vaccine is a safe, effective way to prevent chickenpox and its possible complications.
The procedure was performed under wrist block regional anesthesia with tourniquet control. A single Chinese finger trap was used on the thumb with 5 to 8 lb of ongitudinal traction. The arm was held down with wide tape around the tourniquet securing it to the hand table to serve as countertraction. A shoulder holder, rather than a traction tower, was used to facilitate fluoroscopic intervention more easily. The Trapeziometacarpal joint was detected by palpation. Joint distension was achieved by injecting 1 to 3 mL of normal saline (Fig. 1). It is important to distally direct the needle approximately 20 degrees to clear the dorsal flare of the metacarpal base and enter the joint capsule. This course should be reproduced upon entering with arthroscopic sleeve/ trocar assembly to minimize iatrogenic cartilage injury. Fluid distention is important to facilitate this. The incision for the 1-R (radial) portal, used for proper assessment of the dorsoradial ligament, posterior oblique ligament, and ulnar collateral ligament, was placed just volar to the abductor pollicis longus tendon. The incision for the 1-U (ulnar) portal, for better evaluation of the anterior oblique ligament and ulnar collateral ligament, was made just ulnar to the extensor pollicis brevis tendon. A short-barrel, 1.9-mm, 30- degree inclination arthroscope was used for complete visualization of the CMC joint surfaces, capsule, and ligaments, and then appropriate management was done, as dictated by the stage of the arthritis detected (Fig. 2A). A full-radius mechanical shaver with suction was used in all the cases, particularly for initial debridement and visualization. Most of the cases were augmented with radiofrequency ablation to perform a thorough synovectomy and radiofrequency was also used to perform chondroplasty in the cases with focal articular cartilage wear or fibrillation. Chondroplasty refers to thedebridement of the fibrillated cartilage to improve vascularity of the cartilage and enhance the growth of fibrocartilage. Ligamentous laxity and capsular attenu- ation were treated with thermal capsulorraphy using a radiofrequency shrinkage probe. We were careful to avoid thermal necrosis; hence, a striping technique was used to tighten the capsule of the lax joints. The striping technique refers to thermal shrinkage performed in longitudinal stripes on the lax capsule, so as to leave vascular zones between the stripes; hence, thermal necrosis is prevented. Arthroscopic stage I disease was characterized by synovitis without any cartilage wear, wherein a synovectomy coupled with thermal capsulor- raphy as described was performed.

Infant Airway Obstruction and how to deal with
