- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Eric knew he needed help when an old knee injury began worsening over the course of time and was significantly affecting his quality of life. That’s when he turned to his hometown orthopedic experts at Mayo Clinic Health System in Mankato, who recommended a total knee replacement. After overcoming some initial fears, Eric decided it was time to have the operation — a fuller and more active life with his family depended on it.

Shoulder Injection

Simple Interrupted Pattern Suture
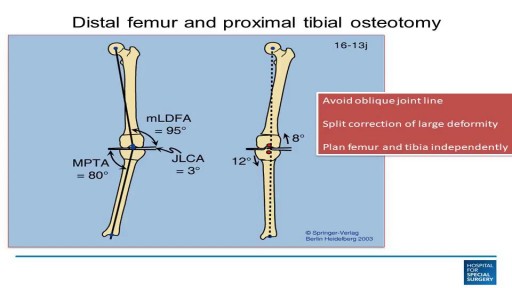
This video discusses knee arthritis, and when to do osteotomy, partial knee replacement, or total knee replacement.

This 25 year young female wanted her split earlobe hole to be repaired.Ear lobe ring hole usually elongated due to continuous use of fancy heavy ear rings.most young ladies suffer from this problem, subsequently this get converted to complete split ear lobe.This needs surgical repair only.This is a cosmetic repair .watch the video , how this repair is done.Usually the split is completely closed with suture.After healing new hole to be done little distance from the repair site.
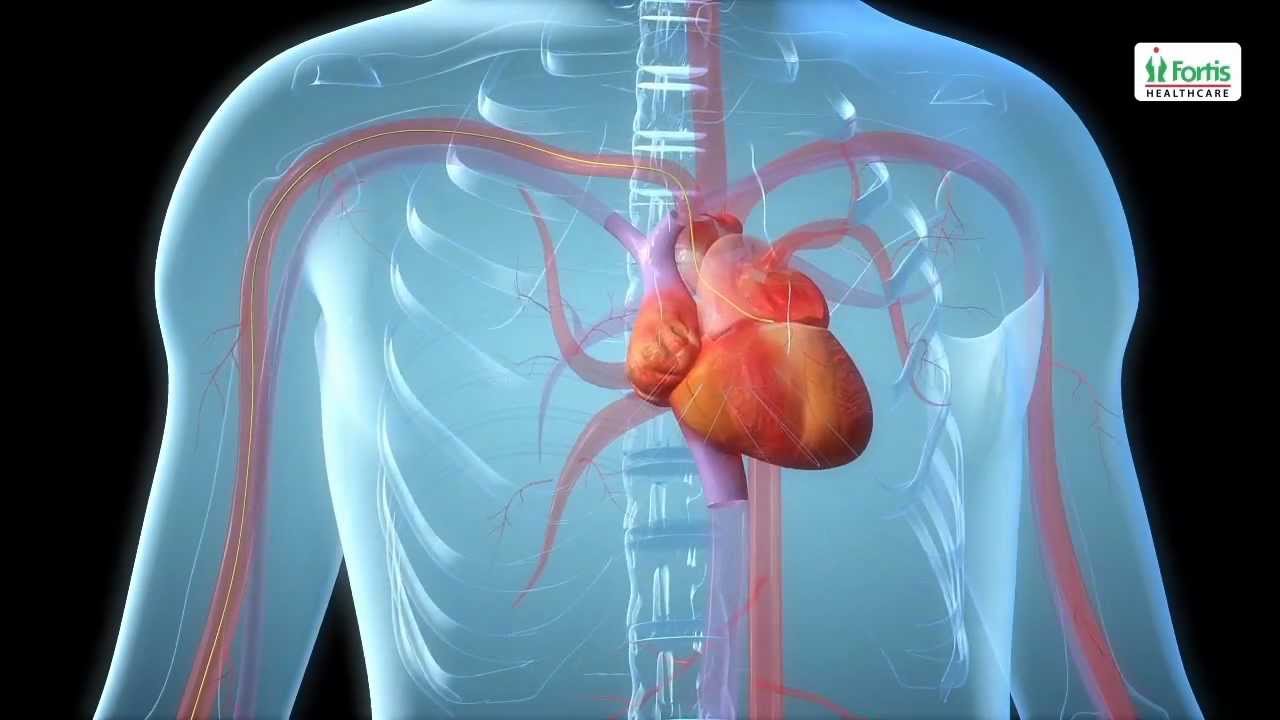
Angioplasty Procedure Animation Video
Emergency angioplasty is an operation that is performed directly after a heart attack, on admission to the hospital. It involves the insertion of a catheter into the blocked blood vessel that caused the heart attack. This opens it up and allows blood to flow again, thus minimizing damage to the heart.
If one or more arteries become clogged, it may result in a heart attack. This normally presents with chest pain, sweating and a feeling of anxiety, among other symptoms. Urgent medical assistance should be sought. A heart attack is a medical emergency requiring intervention as soon as possible.
Know more: http://www.emergencyangioplasty.com/
The procedure was performed under wrist block regional anesthesia with tourniquet control. A single Chinese finger trap was used on the thumb with 5 to 8 lb of ongitudinal traction. The arm was held down with wide tape around the tourniquet securing it to the hand table to serve as countertraction. A shoulder holder, rather than a traction tower, was used to facilitate fluoroscopic intervention more easily. The Trapeziometacarpal joint was detected by palpation. Joint distension was achieved by injecting 1 to 3 mL of normal saline (Fig. 1). It is important to distally direct the needle approximately 20 degrees to clear the dorsal flare of the metacarpal base and enter the joint capsule. This course should be reproduced upon entering with arthroscopic sleeve/ trocar assembly to minimize iatrogenic cartilage injury. Fluid distention is important to facilitate this. The incision for the 1-R (radial) portal, used for proper assessment of the dorsoradial ligament, posterior oblique ligament, and ulnar collateral ligament, was placed just volar to the abductor pollicis longus tendon. The incision for the 1-U (ulnar) portal, for better evaluation of the anterior oblique ligament and ulnar collateral ligament, was made just ulnar to the extensor pollicis brevis tendon. A short-barrel, 1.9-mm, 30- degree inclination arthroscope was used for complete visualization of the CMC joint surfaces, capsule, and ligaments, and then appropriate management was done, as dictated by the stage of the arthritis detected (Fig. 2A). A full-radius mechanical shaver with suction was used in all the cases, particularly for initial debridement and visualization. Most of the cases were augmented with radiofrequency ablation to perform a thorough synovectomy and radiofrequency was also used to perform chondroplasty in the cases with focal articular cartilage wear or fibrillation. Chondroplasty refers to thedebridement of the fibrillated cartilage to improve vascularity of the cartilage and enhance the growth of fibrocartilage. Ligamentous laxity and capsular attenu- ation were treated with thermal capsulorraphy using a radiofrequency shrinkage probe. We were careful to avoid thermal necrosis; hence, a striping technique was used to tighten the capsule of the lax joints. The striping technique refers to thermal shrinkage performed in longitudinal stripes on the lax capsule, so as to leave vascular zones between the stripes; hence, thermal necrosis is prevented. Arthroscopic stage I disease was characterized by synovitis without any cartilage wear, wherein a synovectomy coupled with thermal capsulor- raphy as described was performed.

HD Gynecomastia Surgery
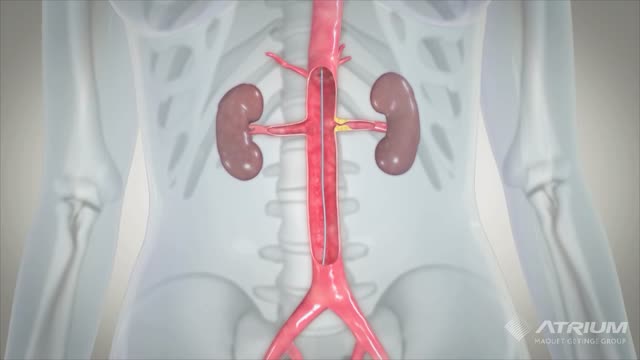
A ureteral stent, sometimes as well called ureteric stent, is a thin tube inserted into the ureter to prevent or treat obstruction of the urine flow from the kidney. The length of the stents used in adult patients varies between 24 to 30 cm.
USMLE Step 2 CS - NOSE BLEEDS This is just preview video. To get full access please visit our website : www.usmletutoring.com

STITCHES: Cleaning, Numbing, & Suturing the Wound
Glaucoma Pathogenesis Simplified
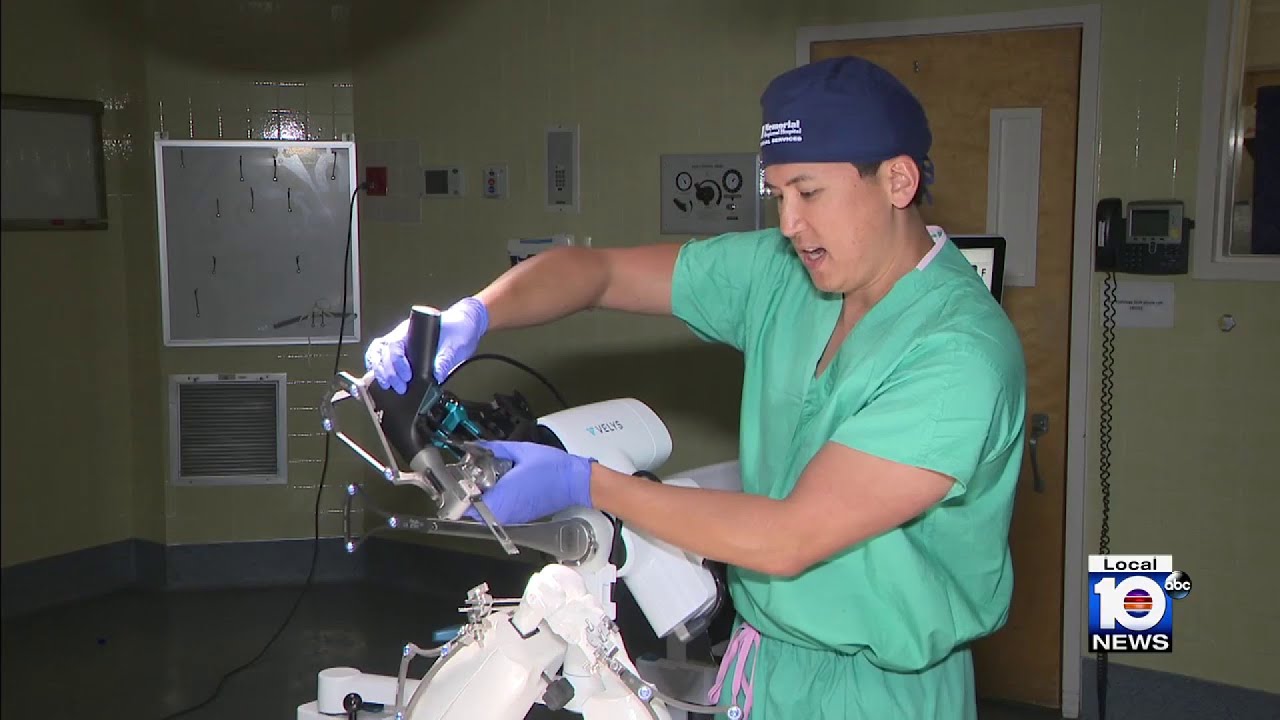
An estimated 900,000 knee replacements are performed in the U.S. every year, but experts say about 15% of patients aren’t totally pleased with the outcome. An advancement in technology is focused on improving those outcomes.

urgical management of proximal humerus fractures may be categorized either according to fracture type (eg, Neer type, anatomic type, greater tuberosity, surgical neck, anatomic neck, articular surface, lesser tuberosity fragments) or according to method of fixation (eg, closed reduction with no fixation, percutaneous fixation, open reduction with internal fixation [ORIF], humeral head replacement associated with tuberosity fixation
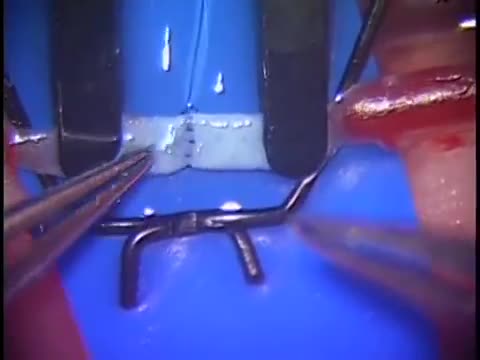
Simple microinstruments and a medical school laboratory microscope were used for anastomosis training. Chicken blood vessels were used as a material for this study. A long segment of blood vessel from the proximal brachial artery to the distal radial artery was used for training. End-to-side anastomosis was practiced first, and the training continued with end-to-end anastomosis of the appropriate segments.

Early Signs that Cancer is Growing in Your Body

Anatomy of The Upper Limb Joints

We will show how to know if you have a sports hernia. These are a few tests you can do on your own. Lower abdominal pain and tightness that increases with twisting and kicking. Stretching and exercises tend to make the discomfort increase.
Want more info? We have a free webinar that covers hip, groin, adductor, lower abdominal strains and sports hernia diagnosis in detail. Use this link to get access. https://bit.ly/37thtNF
#sportshernia #hernia #hippain
To work with us, contact us using this link https://bit.ly/3zCBnzZ or call us 714-502-4243. We have online programs, virtual and in-person options.
Costa Mesa, CA www.p2sportscare.com
Option 1: Groin On-Demand Webinar https://bit.ly/37thtNF
Option 2: Video Guide https://bit.ly/33aLIqC
Option 3 (the best): Work With Us https://www.p2sportscare.com/
Sports Hernia Diagnosis
What Is A Sports Hernia?
A sports hernia is tearing of the transversalis fascia of the lower abdominal or groin region. A common misconception is that a sports hernia is the same as a traditional hernia. The mechanism of injury is rapid twisting and change of direction within sports, such as football, basketball, soccer and hockey.
The term “sports hernia” is becoming mainstream with more professional athletes being diagnosed. The following are just to name a few:
Torii Hunter
Tom Brady
Ryan Getzlaf
Julio Jones
Jeremy Shockey
If you follow any of these professional athletes, they all seem to have the same thing in common: Lingering groin pain. If you play fantasy sports, this is a major headache since it seems so minor, but it can land a player on Injury Reserve on a moments notice. In real life, it is a very frustrating condition to say the least. It is hard to pin point, goes away with rest and comes back after activity, but is hardly painful enough to make you want to stop. It lingers and is always on your mind. And if you’re looking for my step-by-step sports hernia rehab video course here it is.
One the best definitions of Sport hernias is the following by Harmon:
The phenomena of chronic activity–related groin pain that it is unresponsive to conservative therapy and significantly improves with surgical repair.”
This is truly how sports hernias behave in a clinical setting. It is not uncommon for a sports hernia to be unrecognized for months and even years. Unlike your typical sports injury, most sports medicine offices have only seen a handful of cases. It’s just not on most doctors’ radar. The purpose of this article is not only to bring awareness about sports hernias, but also to educate.
Will you find quick fixes in this article for sports hernia rehab?
Nope. There is no quick fix for this condition, and if someone is trying to sell you one, they are blowing smoke up your you-know-what.
Is there a way to decrease the pain related to sports hernias?
Yes. Proper rehab and avoidance of activity for a certain period of time will assist greatly, but this will not always stop it from coming back. Pain is the first thing to go and last thing to come. Do not be fooled when you become pain-free by resting it. Pain is only one measure of improvement in your rehab. Strength, change of direction, balance and power (just to name a few) are important, since you obviously desire to play your sport again. If you wanted to be a couch potato, you would be feeling better in no time. Watching Sports Center doesn’t require any movement.
Why is this article so long?
There is a lot of information on sports hernias available to you on the web. However, much of the information is spread out all over the internet and hard for athletes to digest due to complicated terminology. This article lays out the foundational terminology you will need to understand what options you have with your injury. We will go over anatomy, biomechanics, rehab, surgery, and even the fun facts. The information I am using is from the last ten years of medical research, up until 2016. We will be making updates overtime when something new is found as well. So link to this page and share with friends. This is the best source for information on sports hernias you will find.
Common Names (or Aliases?) for Sports Hernias
Sportsman’s Hernia
Athletic Pubalgia
Gilmore’s Groin
How Do You Know If You Have A Sports Hernia?
Typical athlete characteristics:
Male, age mid-20s
Common sports: soccer, hockey, tennis, football, field hockey
Motions involved: cutting, pivoting, kicking and sharp turns
Gradual onset
How A Sports Hernia Develops
Chronic groin pain typically happens over time, which is why with sports hernias, we do not hear many stories of feeling a “pop” or a specific moment of injury. It is the result of “overuse” mechanics stemming from a combination of inadequate strength and endurance, lack of dynamic control, movement pattern abnormalities, and discoordination of motion in the groin area.
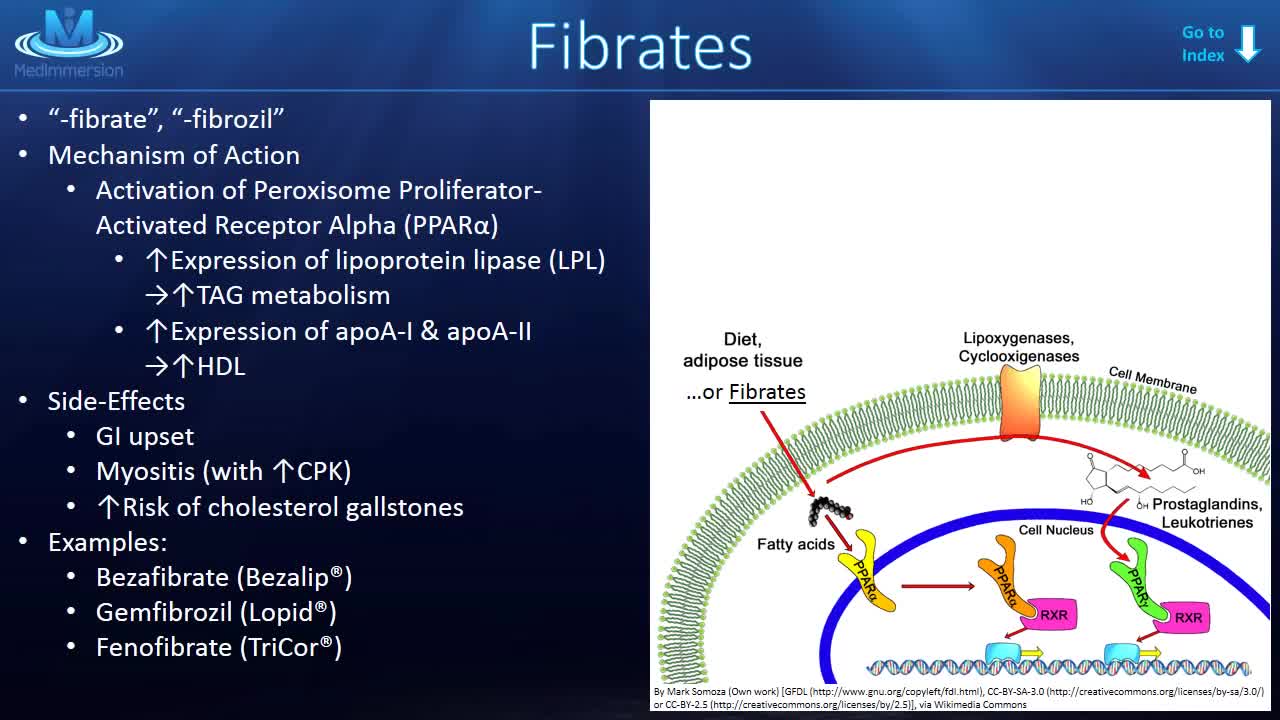
Lipid-Lowering Agents HMG-CoA reductase inhibitors (statins) These agents inhibit the rate-limiting step in cholesterol biosynthesis by competitively inhibiting HMG-CoA reductase. Note the following: Low-density lipoprotein (LDL) reduction of 25%-60% Examples include Atorvastatin, fluvastatin, lovastatin, pitavastatin, pravastatin, rosuvastatin, simvastatin Contraindications include hypersensitivity, active liver disease, pregnancy, lactation, coadministration with strong CYP3A4 inhibitors (selected statins) Vitamin B3 Vitamin B3 inhibits very-low-density lipoprotein (VLDL) synthesis. Note the following: LDL reduction of 10% High-density lipoprotein (HDL) increase of 20% Example includes Niacin (nicotinic acid) Contraindications include hypersensitivity, liver disease, active peptic ulcer, severe hypotension, arterial bleeding Fibrates Fibrates enhance lipoprotein lipase, resulting in increased VLDL catabolism, fatty acid oxidation, and triglycerides elimination. They decrease hepatic extraction of free fatty acids. Note the following: LDL reduction of 15% Triglyceride reduction of 35% Examples include Gemfibrozil, fenofibrate, fenofibrate (micronized), fenofibric acid Contraindications include active liver disease, renal disease, primary biliary cirrhosis, gallbladder disease 2-Azetidiones These agents inhibit sterol transporter at brush border and, consequently, intestinal absorption of cholesterol. LDL reduction of 15% Example includes Ezetimibe Contraindications include hypersensitivity, coadministration with statins (if active liver disease) Bile acid sequestrants These agents lower cholesterol and LDL via bile duct sequestration. Note the following: LDL reduction of 15% Examples include Cholestyramine, colesevelam, colestipol Contraindications include biliary/bowel obstruction, serum triglycerides >300-500 mg/dL, history of hypertriglyceridemia-induced pancreatitis

Watch that video to know How to get Pregnant Fast
