- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Unruptured Aneurysms: When and How to Treat
Lumbar puncture is a common emergency department procedure used to obtain information about the cerebrospinal fluid (CSF) for diagnostic and, less commonly, therapeutic reasons. Please refer to the full article on Lumbar Puncture for more details on the lumbar puncture procedure. Lumbar puncture is typically performed via “blind” surface landmark guidance. The surface landmark technique is reported to be successful in a high percentage of attempted lumbar punctures; however, surface landmark identification of underlying structures has been shown to be accurate only 30% of the time. [1] Unsuccessful identification of proper landmarks often leads to increased difficulty in obtaining CSF, if the procedure is performed, and a higher rate of complications. Few alternatives are available in these cases. If available, fluoroscopic-guided lumbar puncture may be performed. If not, treatment is sometimes initiated empirically without obtaining CSF. Disadvantages of using fluoroscopy include limited availability or necessary transport of the patient outside of the emergency department, inability to directly visualize the spinal canal, and inherent radiation exposure

TPE removes large-molecular-weight substances such as harmful antibodies from the plasma. It is usually carried out using an automated blood cell separator to ensure fluid balance and maintain a normal plasma volume. This may require the insertion of a femoral or jugular line to allow adequate blood flow. Typically, 30–40 mL/kg of plasma (1–1.5 plasma volumes) are removed at each procedure and replaced with isotonic 4.5 or 5.0% human albumin solution (some services substitute 25–50% of replacement volume with 0.9% saline). Exchange with fresh frozen plasma (FFP) is reserved for the replacement of ADAMTS13 in thrombotic thrombocytopenic purpura (see below) or to replace clotting factors. A one plasma volume exchange removes about 66% of an intravascular constituent and a two plasma volume exchange approximately 85%. TPE is normally combined with disease modifying treatment, such as immunosuppressive drugs, for the underlying condition.

A laparoscope is a small, thin tube that is put into your body through a tiny cut made just below your navel. Your surgeon can then see your gallbladder on a television screen and do the surgery with tools inserted in three other small cuts made in the right upper part of your abdomen. Your gallbladder is then taken out through one of the incisions.

Colonoscopy Showing Moving Parasites

What is Esophageal Dilation?
Esophageal dilation is a procedure that allows your doctor to dilate, or stretch, a narrowed area of your esophagus [swallowing tube]. Doctors can use various techniques for this procedure. Your doctor might perform the procedure as part of a sedated endoscopy. Alternatively, your doctor might apply a local anesthetic spray to the back of your throat and then pass a weighted dilator through your mouth and into your esophagus.
Why is it Done?
The most common cause of narrowing of the esophagus, or stricture, is scarring of the esophagus from reflux of acid occurring in patients with heartburn. Patients with a narrowed portion of the esophagus often have trouble swallowing; food feels like it is "stuck" in the chest region, causing discomfort or pain. Less common causes of esophageal narrowing are webs or rings (which are thin layers of excess tissue), cancer of the esophagus, scarring after radiation treatment or a disorder of the way the esophagus moves [motility disorder].
How Should I Prepare for the Procedure?
An empty stomach allows for the best and safest examination, so you should have nothing to drink, including water, for at least six hours before the examination. Your doctor will tell you when to start fasting.
Tell your doctor in advance about any medications you take, particularly aspirin products or anticoagulants (blood thinners). Most medications can be continued as usual, but you might need to adjust your usual dose before the examination. Your doctor will give you specific guidance. Tell your doctor if you have any allergies to medications as well as medical conditions such as heart or lung disease. Also, tell your doctor if you require antibiotics prior to dental procedures, because you might need antibiotics prior to esophageal dilation as well.
What Can I Expect during Esophageal Dilation?
Your doctor might perform esophageal dilation with sedation along with an upper endoscopy. Your doctor may spray your throat with a local anesthetic spray, and then give you sedatives to help you relax. Your doctor then will pass the endoscope through your mouth and into the esophagus, stomach and duodenum. The endoscope does not interfere with your breathing. At this point your doctor will determine whether to use a dilating balloon or plastic dilators over a guiding wire to stretch your esophagus. You might experience mild pressure in the back of your throat or in your chest during the procedure. Alternatively, your doctor might start by spraying your throat with a local anesthetic. Your doctor will then pass a tapered dilating instrument through your mouth and guide it into the esophagus.
What Can I Expect after Esophageal Dilation?
After the dilation is done, you will probably be observed for a short period of time and then allowed to return to your normal activities. You may resume drinking when the anesthetic no longer causes numbness to your throat, unless your doctor instructs you otherwise. Most patients experience no symptoms after this procedure and can resume eating the next day, but you might experience a mild sore throat for the remainder of the day.
If you received sedatives, you probably will be monitored in a recovery area until you are ready to leave. You will not be allowed to drive after the procedure even though you might not feel tired. You should arrange for someone to accompany you home, because the sedatives might affect your judgment and reflexes for the rest of the day.
What are the Potential Complications of Esophageal Dilation?
Although complications can occur even when the procedure is performed correctly, they are rare when performed by doctors who are specially trained. A perforation, or hole, of the esophagus lining occurs in a small percentage of cases and may require surgery. A tear of the esophagus lining may occur and bleeding may result. Complications from heart or lung diseases are potential risks
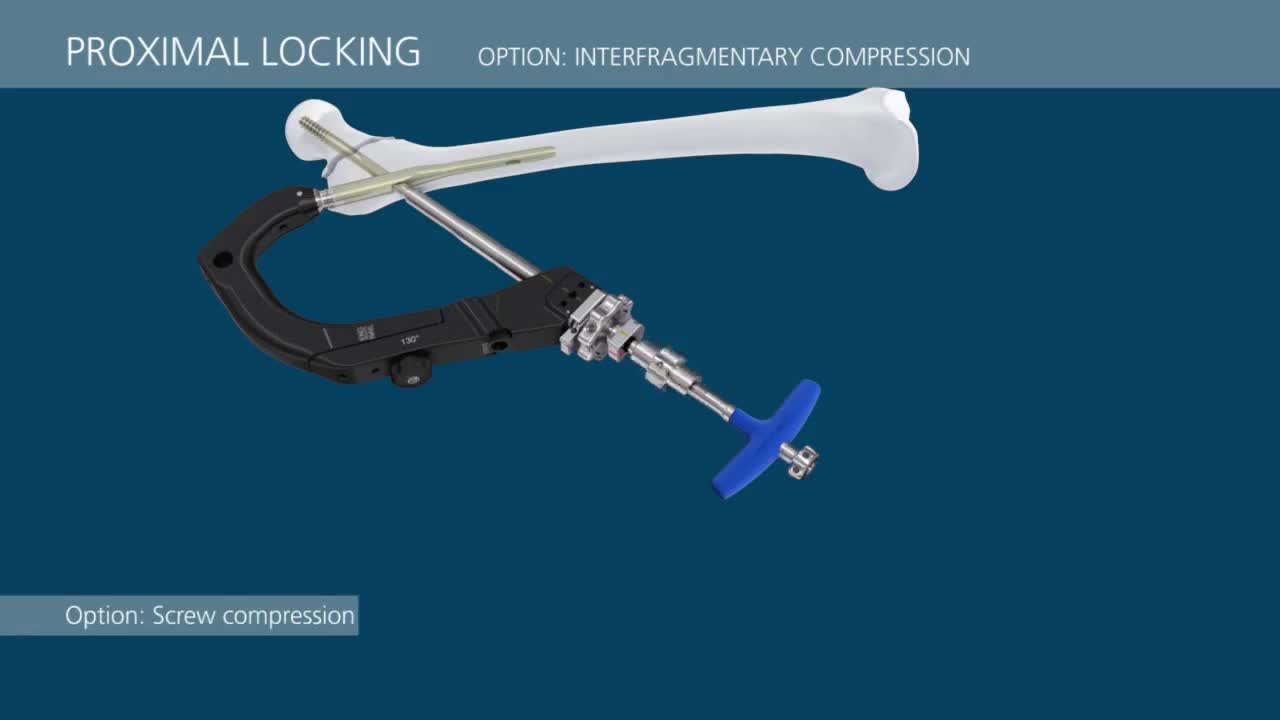
This video demonstrates a step-by-step technique for using the TFN-Advanced™ Proximal Femoral Nailing System (TFNA).

Examination of Cranial nerve VIII: vestibulocochlear

a video showing the correct position for needle holding

LASIK is one of the most popular elective surgeries in the United States with 95% of patients walking away satisfied with their vision, according to one FDA study. But like with any surgery, there are risks.

Capsulorrhexis after trypan blue staining of anterior capsule. Controlled Rhexis with forceps. Phacoemulsification by devide and conquer technique

If you have gestational diabetes, your baby may be at increased risk of: Excessive birth weight. Extra glucose in your bloodstream crosses the placenta, which triggers your baby's pancreas to make extra insulin. This can cause your baby to grow too large (macrosomia).


This video demonstrates how a broken nose is fixed using only local anesthesia and without sedation. Of course, this can also be performed while asleep.
USMLE Step 2 CS - Vaginal Discharge This is just preview video. To get full access please visit our website : www.usmletutoring.com

Watch that video of a Very Large Mole Removal Surgery

Most scoliosis surgeons agree that children who have very severe curves (45-50° and higher) will need surgery to lessen the curve and prevent it from getting worse. The operation for scoliosis is a spinal fusion. The basic idea is to realign and fuse together the curved vertebrae so that they heal into a single, solid bone. With the tools and technology available today, scoliosis surgeons are able to improve curves significantly.

Perineal repair after episiotomy or spontaneous obstetric laceration is one of the most common surgical procedures. Potential sequelae of obstetric perineal lacerations include chronic perineal pain,1 dyspareunia,2 and urinary and fecal incontinence.3–5 Few studies of laceration repair techniques exist to support the development of an evidence-based approach to perineal repair. This article discusses a repair method that emphasizes anatomic detail, with the expectation that an anatomically correct perineal repair may result in a better long-term functional outcome.

A fluid-filled swelling (cyst) in the Bartholin's glands, which lubricate the vagina.

Stop Nose Bleeds by Cautery
