- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

39 Yr. Male with Aortic Stenosis and Incompetance and Good LV Function. The Patient is an athlete and did not want to take oral anticoagulants so opted out for a Bio-prosthesis. A 23mm Hancock II Porcine Xenograft was used in this operation. Usually central aortic and Rt. Atrial cannulation is per...formed with this procedure, however on occasions Percutaneous (Seldinger Technique) Femoro Femoral artery cannulation is used. The Kit is manufactured by DLP and consists of a 20mm Arterial cannula and a 29mm two stage Rt. Atrial Cannula.

Capsaicin binds to pain receptors on our nerves called TRPV1. Normally, it reacts to heat by sending warning signals to the brain. Capsaicin causes TRPV1 to send those same signals. So, you react as if there's something hot in your mouth
procedure is usually done in the hospital or outpatient surgical center under general anesthesia (while you are asleep and pain-free). The procedure is performed in the following way: The surgeon makes a small cut (incision) below the belly button (navel). A needle or tube is inserted into the incision. Carbon dioxide gas is passed into the abdomen through the needle or tube. The gas helps expand the area, giving the surgeon more room to work, and helping the surgeon see the organs more clearly. A tube is placed through the cut in your abdomen. A tiny video camera (laparoscope) goes through this tube and is used to see the inside of your pelvis and abdomen. More small cuts may be made if other instruments are needed to get a better view of certain organs. If you are having gynecologic laparoscopy, dye may be injected into your cervix area so the surgeon can view your fallopian tubes. After the exam, the gas, laparoscope, and instruments are removed, and the cuts are closed. You will have bandages over those areas.
Watch that video of Removing Worms and Parasites From Girl's Mouth
You may have recently found out that you are deficient or know someone who is. It's shocking for most people when they have never had a problem before and believe nothing has changed to make it a problem now. The truth is that a lot has changed, and vitamin D deficiency and insufficiency is now a global public-health problem affecting an estimated 1 billion people worldwide. The most well-known consequences to not having enough vitamin D are rickets in children and osteomalacia in adults. These are far from the only problems associated with a vitamin D deficiency.

This surgical procedure helps children defeat bone cancer.
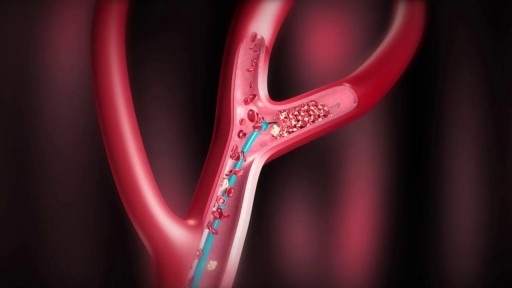
Diagnosis To determine the most appropriate treatment for your stroke, your emergency team needs to evaluate the type of stroke you're having and the areas of your brain affected by the stroke. They also need to rule out other possible causes of your symptoms, such as a brain tumor or a drug reaction. Your doctor may use several tests to determine your risk of stroke, including: Stroke consultation Stroke consultation Stroke consultation at Mayo Clinic Brain tissue damaged by stroke CT scan of brain tissue damaged by stroke Cerebral angiogram Cerebral angiogram Physical examination. Your doctor will ask you or a family member what symptoms you've been having, when they started and what you were doing when they began. Your doctor then will evaluate whether these symptoms are still present. Your doctor will want to know what medications you take and whether you have experienced any head injuries. You'll be asked about your personal and family history of heart disease, transient ischemic attack and stroke. Your doctor will check your blood pressure and use a stethoscope to listen to your heart and to listen for a whooshing sound (bruit) over your neck (carotid) arteries, which may indicate atherosclerosis. Your doctor may also use an ophthalmoscope to check for signs of tiny cholesterol crystals or clots in the blood vessels at the back of your eyes. Blood tests. You may have several blood tests, which tell your care team how fast your blood clots, whether your blood sugar is abnormally high or low, whether critical blood chemicals are out of balance, or whether you may have an infection. Managing your blood's clotting time and levels of sugar and other key chemicals will be part of your stroke care. Computerized tomography (CT) scan. A CT scan uses a series of X-rays to create a detailed image of your brain. A CT scan can show a hemorrhage, tumor, stroke and other conditions. Doctors may inject a dye into your bloodstream to view your blood vessels in your neck and brain in greater detail (computerized tomography angiography). There are different types of CT scans that your doctor may use depending on your situation. Magnetic resonance imaging (MRI). An MRI uses powerful radio waves and magnets to create a detailed view of your brain. An MRI can detect brain tissue damaged by an ischemic stroke and brain hemorrhages. Your doctor may inject a dye into a blood vessel to view the arteries and veins and highlight blood flow (magnetic resonance angiography, or magnetic resonance venography). Carotid ultrasound. In this test, sound waves create detailed images of the inside of the carotid arteries in your neck. This test shows buildup of fatty deposits (plaques) and blood flow in your carotid arteries. Cerebral angiogram. In this test, your doctor inserts a thin, flexible tube (catheter) through a small incision, usually in your groin, and guides it through your major arteries and into your carotid or vertebral artery. Then your doctor injects a dye into your blood vessels to make them visible under X-ray imaging. This procedure gives a detailed view of arteries in your brain and neck. Echocardiogram. An echocardiogram uses sound waves to create detailed images of your heart. An echocardiogram can find a source of clots in your heart that may have traveled from your heart to your brain and caused your stroke. You may have a transesophageal echocardiogram. In this test, your doctor inserts a flexible tube with a small device (transducer) attached into your throat and down into the tube that connects the back of your mouth to your stomach (esophagus). Because your esophagus is directly behind your heart, a transesophageal echocardiogram can create clear, detailed ultrasound images of your heart and any blood clots. Treatment Emergency treatment for stroke depends on whether you're having an ischemic stroke blocking an artery — the most common kind — or a hemorrhagic stroke that involves bleeding into the brain. Ischemic stroke To treat an ischemic stroke, doctors must quickly restore blood flow to your brain. Emergency treatment with medications. Therapy with clot-busting drugs must start within 4.5 hours if they are given into the vein — and the sooner, the better. Quick treatment not only improves your chances of survival but also may reduce complications. You may be given: Intravenous injection of tissue plasminogen activator (tPA). This injection of recombinant tissue plasminogen activator (tPA), also called alteplase, is considered the gold standard treatment for ischemic stroke. An injection of tPA is usually given through a vein in the arm. This potent clot-busting drug ideally is given within three hours. In some instances, tPA can be given up to 4.5 hours after stroke symptoms begin. This drug restores blood flow by dissolving the blood clot causing your stroke, and it may help people who have had strokes recover more fully. Your doctor will consider certain risks, such as potential bleeding in the brain, to determine if tPA is appropriate for you. Emergency endovascular procedures. Doctors sometimes treat ischemic strokes with procedures performed directly inside the blocked blood vessel. These procedures must be performed as soon as possible, depending on features of the blood clot: Medications delivered directly to the brain. Doctors may insert a long, thin tube (catheter) through an artery in your groin and thread it to your brain to deliver tPA directly into the area where the stroke is occurring. This is called intra-arterial thrombolysis. The time window for this treatment is somewhat longer than for intravenous tPA, but is still limited. Removing the clot with a stent retriever. Doctors may use a catheter to maneuver a device into the blocked blood vessel in your brain and trap and remove the clot. This procedure is particularly beneficial for people with large clots that can't be completely dissolved with tPA, though this procedure is often performed in combination with intravenous tPA. Several large and recent studies suggest that, depending on the location of the clot and other factors, endovascular therapy might be the most effective treatment. Endovascular therapy has been shown to significantly improve outcomes and reduce long-term disability after ischemic stroke. Other procedures. To decrease your risk of having another stroke or transient ischemic attack, your doctor may recommend a procedure to open up an artery that's narrowed by plaque. Doctors sometimes recommend the following procedures to prevent a stroke. Options will vary depending on your situation: Carotid endarterectomy. In a carotid endarterectomy, a surgeon removes plaques from arteries that run along each side of your neck to your brain (carotid arteries). In this procedure, your surgeon makes an incision along the front of your neck, opens your carotid artery and removes plaque that blocks the carotid artery. Your surgeon then repairs the artery with stitches or a patch made from a vein or artificial material (graft). The procedure may reduce your risk of ischemic stroke. However, a carotid endarterectomy also involves risks, especially for people with heart disease or other medical conditions. Angioplasty and stents. In an angioplasty, a surgeon usually accesses your carotid arteries through an artery in your groin. Here, your surgeon can gently and safely navigate to the carotid arteries in your neck. A balloon is then inflated to expand the narrowed artery. Then a stent can be inserted to support the opened artery. Hemorrhagic stroke Emergency treatment of hemorrhagic stroke focuses on controlling your bleeding and reducing pressure in your brain. You might also need surgery to help reduce future risk. Emergency measures. If you take warfarin (Coumadin, Jantoven) or anti-platelet drugs such as clopidogrel (Plavix) to prevent blood clots, you may be given drugs or transfusions of blood products to counteract the blood thinners' effects. You may also be given drugs to lower pressure in your brain (intracranial pressure), lower your blood pressure, prevent vasospasm or prevent seizures. Once the bleeding in your brain stops, treatment usually involves supportive medical care while your body absorbs the blood. Healing is similar to what happens while a bad bruise goes away. If the area of bleeding is large, your doctor may perform surgery to remove the blood and relieve pressure on your brain. Surgical blood vessel repair. Surgery may be used to repair blood vessel abnormalities associated with hemorrhagic strokes. Your doctor may recommend one of these procedures after a stroke or if an aneurysm or arteriovenous malformation (AVM) or other type of vascular malformation caused your hemorrhagic stroke: Surgical clipping. A surgeon places a tiny clamp at the base of the aneurysm, to stop blood flow to it. This clamp can keep the aneurysm from bursting, or it can prevent re-bleeding of an aneurysm that has recently hemorrhaged. Coiling (endovascular embolization). A surgeon inserts a catheter into an artery in your groin and guides it to your brain using X-ray imaging. Tiny detachable coils are guided into the aneurysm (aneurysm coiling). The coils fill the aneurysm, which blocks blood flow into the aneurysm and causes the blood to clot. Surgical AVM removal. Surgeons may remove a smaller AVM if it's located in an accessible area of your brain, to eliminate the risk of rupture and lower the risk of hemorrhagic stroke. However, it's not always possible to remove an AVM if its removal would cause too large a reduction in brain function, or if it's large or located deep within your brain. Stereotactic radiosurgery. Using multiple beams of highly focused radiation, stereotactic radiosurgery is an advanced minimally invasive treatment used to repair vascular malformations. Stroke recovery and rehabilitation Brain hemisphere connections Brain hemisphere connections After emergency treatment, stroke care focuses on helping you recover as much function as possible and return to independent living. The impact of your stroke depends on the area of the brain involved and the amount of tissue damaged. If your stroke affected the right side of your brain, your movement and sensation on the left side of your body may be affected. If your stroke damaged the brain tissue on the left side of your brain, your movement and sensation on the right side of your body may be affected. Brain damage to the left side of your brain may cause speech and language disorders. In addition, if you've had a stroke, you may have problems with breathing, swallowing, balancing and vision. Most stroke survivors receive treatment in a rehabilitation program. Your doctor will recommend the most rigorous therapy program you can handle based on your age, overall health and degree of disability from your stroke. Your doctor will take into consideration your lifestyle, interests and priorities, and the availability of family members or other caregivers. Your rehabilitation program may begin before you leave the hospital. After discharge, you might continue your program in a rehabilitation unit of the same hospital, another rehabilitation unit or skilled nursing facility, an outpatient unit, or your home. Every person's stroke recovery is different. Depending on your condition, your treatment team may include: Doctor trained in brain conditions (neurologist) Rehabilitation doctor (physiatrist) Nurse Dietitian Physical therapist Occupational therapist Recreational therapist Speech pathologist Social worker Case manager Psychologist or psychiatrist Chaplain Speech therapy session Speech therapy is often a part of stroke rehabilitation. Treatment outcomes One way to evaluate the care of patients diagnosed with stroke is to look at the percentage of patients receiving the timely and effective care measures that are appropriate. The goal is 100 percent. The graphs below display the percentage of eligible Mayo Clinic patients diagnosed with stroke receiving all of the appropriate care measures.
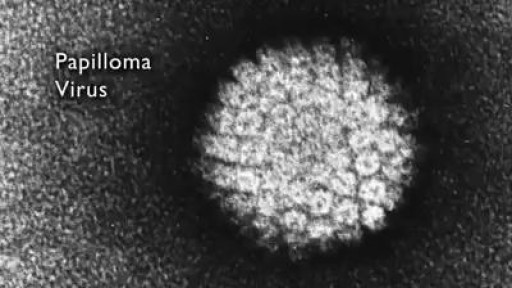
A short story about Warts, Are they contagious?

Learn one of the hidden reasons why you still have a thyroid symptoms. If your lab results are "normal"--then why do you still have thyroid symptoms like: * Tired, sluggish * Can't lose weight even with exercise * Feel cold—hands, feet, or all over * Require excessive amounts of sleep to function properly * Increase in weight gain even with low-calorie diet * Gain weight easily * Difficult, infrequent bowel movements * Depression, lack of motivation * Morning headaches that wear off as the day progresses * Outer third of eyebrow thins * Thinning of hair on scalp, face or genitals or hair loss * Dryness of skin and/or scalp * Mental sluggishness * Nervousness and emotional * Insomnia * Night sweats

new study about the size of penis
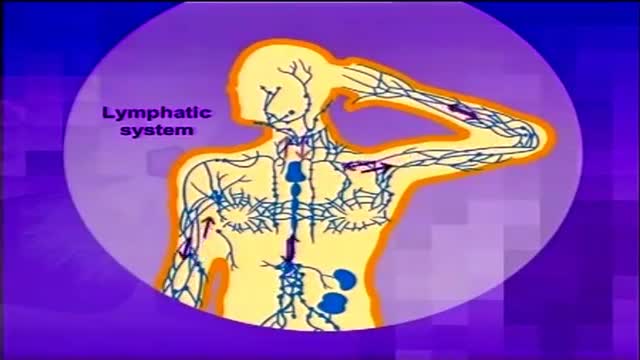
Lymphoma is cancer of the lymph system (or lymphatic system), which is part of our immunity. It is characterized by the formation of solid tumors in the immune system.1 The cancer affects immune cells called lymphocytes, which are white blood cells. Diagram of the lymphatic system The lymphatic system is a system of vessels that branch back from virtually all our tissues to drain excess fluids and present foreign material to the lymph nodes. Learn more about the lymphatic system here. Statistics from the US National Cancer Institute estimate that there are nearly 20 cases of non-Hodgkin's lymphoma for every 100,000 people in the American population.2 Hodgkin's lymphoma, meanwhile, is relatively rare, with around three cases in every 100,000 people.3

A short introduction on how to take a correction impression. The shown materials are recommended by Orthorobot and have proven to be fully compatible with the Orthorobot lab procedure.

In this animated episode of eOrthopodTV, orthopedic surgeon Randale C. Sechrest, MD narrates the procedure to replace an arthritic knee with an artificial joint.

Coolsculpting, for non-invasive fat reduction of the upper arms is now available at Dr.Ron Shelton's Midtown Manhattan office

Pediatric febrile seizures, which represent the most common childhood seizure disorder, exist only in association with an elevated temperature. Evidence suggests, however, that they have little connection with cognitive function, so the prognosis for normal neurologic function is excellent in children with febrile seizures. [1] Epidemiologic studies have led to the division of febrile seizures into 3 groups, as follows: Simple febrile seizures Complex febrile seizures Symptomatic febrile seizures Essential update: Starting MMR/MMRV vaccination earlier may reduce seizure risk In a case-series analysis of a cohort of 323,247 US children born from 2004 to 2008, Hambidge et al found that delaying the first dose of measles-mumps-rubella (MMR) or measles-mumps-rubella-varicella (MMRV) vaccine beyond the age of 15 months may more than double the risk of postvaccination seizures in the second year of life. [2, 3] In infants, there was no association between vaccination timing and postvaccination seizures. [3] In the second year of life, however, the incident rate ratio (IRR) for seizures within 7-10 days was 2.65 (95% confidence interval [CI], 1.99-3.55) after first MMR doses at 12-15 months of age, compared with 6.53 (95% CI, 3.15-13.53) after first MMR doses at 16-23 months. For the MMRV vaccine, the IRR for seizures was 4.95 (95% CI, 3.68-6.66) after first doses at 12-15 months, compared with 9.80 (95% CI, 4.35-22.06) for first doses at 16-23 months.

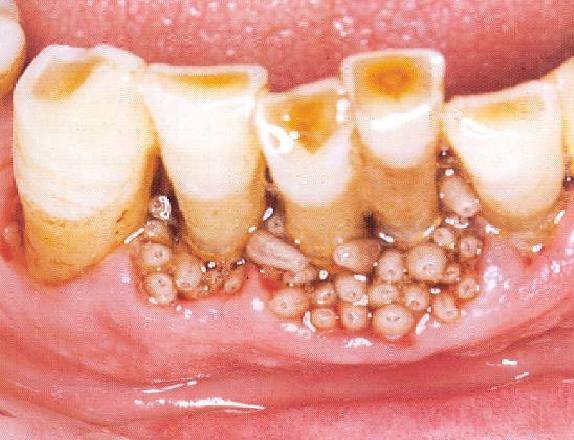
An abscess is a tender mass generally surrounded by a colored area from pink to deep red. Abscesses are often easy to feel by touching. The middle of an abscess is full of pus and debris. Painful and warm to touch, abscesses can show up any place on your body. The most common sites are in your armpits (axillae), areas around your anus and vagina(Bartholin gland abscess), the base of your spine (pilonidal abscess), around a tooth (dental abscess), and in your groin. Inflammation around a hair follicle can also lead to the formation of an abscess, which is called a boil (furuncle).
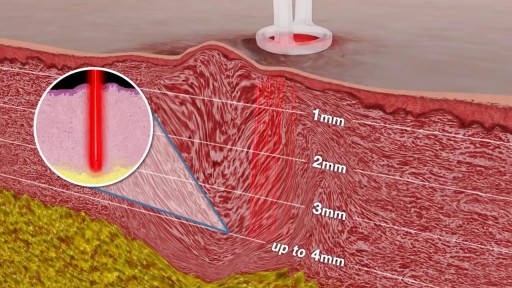
Scar revision includes techniques that improve the appearance of an unsightly scar, regardless of its size, type or age. This is typically not covered by insurance carriers and is treated as a cosmetic procedure. Though scars can never be completely removed, the appearance of scarring can be greatly diminished. Who Should Get Scar Revision? The best candidates for scar revision are in good health and have realistic expectations. Scar revision may be used to treat: Hyperpigmented scars Large or plainly visible scars Keloid scarring Raised scars Deep depression scars After scar revision, the appearance of your scar should be greatly reduced. Scar revision can improve the size, shape and color of your scar. Multiple procedures may be needed to achieve optimal results. There are several different techniques that can be used during your scar revision. During a consultation, we can discuss the best techniques and determine if you are a suitable candidate. What to Expect During Your Scar Revision Your scar revision may involve one or more of the following techniques: Topical treatments (gels, creams, external compression) can treat mild scarring or changes in pigmentation. Injectable treatments like dermal fillers are best for filling in scar depressions. These treatment options can provide long-lasting improvements, however, they are not always permanent. Surface treatments like chemical peels, dermabrasion, laser therapy and skin bleaching can improve skin tone and texture. More than one treatment may be needed to achieve optimal results. Surgical scar revision is only used in more severe cases. Reconstructive techniques like Z-plasty, tissue expansion, or skin grafting replace a prominent scar with a less noticeable scar. After Your Surgery Scar revision recovery varies depending on the procedure you have elected. Topical and injectable treatments rarely require downtime. Surface treatments and surgical removal can require several days of recovery. You may experience some temporary bruising, swelling, or discomfort. Over-the-counter or prescription medication can be used to manage pain. Topical and injectable treatments are likely to require sustained application to maintain results. The final results of surface treatments and surgical removal may not be visible for several weeks to months. It is important to protect the treatment area from direct sun exposure for several weeks. Additional details about your specific recovery will be discussed during your consultation.
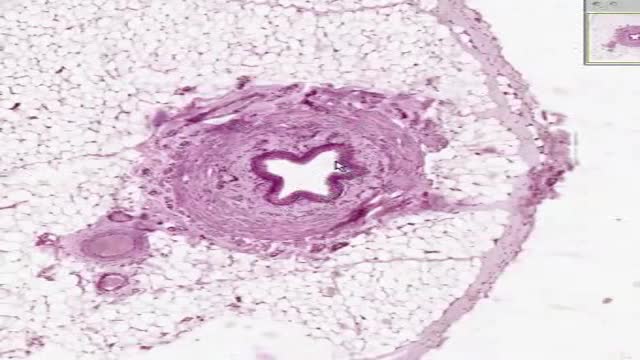
Histology of Ureter
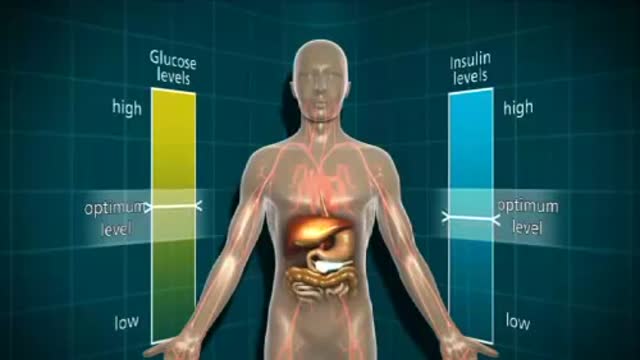
a disease in which the body’s ability to produce or respond to the hormone insulin is impaired, resulting in abnormal metabolism of carbohydrates and elevated levels of glucose in the blood and urine.

Appendectomy (midline caecum)
