- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

To learn more about licensing this video for content marketing or patient education purposes, visit: http://www.nucleushealth.com/?utm_source=youtube&utm_medium=video-description&utm_campaign=stroke-071411
This video, created by Nucleus Medical Media, gives a thorough explanation of stroke, covering anatomy and physiology, different types of stroke, and treatment.
ANH11048
Watch that video to know about the Anal Intercourse Medical Risks

This surgery is usually done while you are under general anesthesia. That means you will be asleep and pain-free. Healthy skin is taken from a place on your body called the donor site. Most people who are having a skin graft have a split-thickness skin graft. This takes the two top layers of skin from the donor site (the epidermis) and the layer under the epidermis (the dermis). The donor site can be any area of the body. Most times, it is an area that is hidden by clothes, such as the buttock or inner thigh. The graft is carefully spread on the bare area where it is being transplanted. It is held in place either by gentle pressure from a well-padded dressing that covers it, or by staples or a few small stitches. The donor-site area is covered with a sterile dressing for 3 to 5 days. People with deeper tissue loss may need a full-thickness skin graft. This requires an entire thickness of skin from the donor site, not just the top two layers. A full-thickness skin graft is a more complicated procedure. Common donor sites for full-thickness skin grafts include the chest wall, back, or abdominal wall.

Diabetes Complications and Kidney Disease

A hematoma is a collection of blood outside of a blood vessel. There are several types of hematomas and they are often described based on their location. Examples of hematomas include subdural, spinal, under the finger or toenail bed (subungual), ear, and liver (hepatic). Some causes of hematomas are as pelvic bone fractures, fingernail injuries (subungual), bumps, passing blood clots, blood clot in the leg (DVT), blood cancers, and excessive alcohol use. Symptoms of hematomas depend upon their location and whether adjacent structures are affected by the inflammation and swelling associated with the bleeding and may include
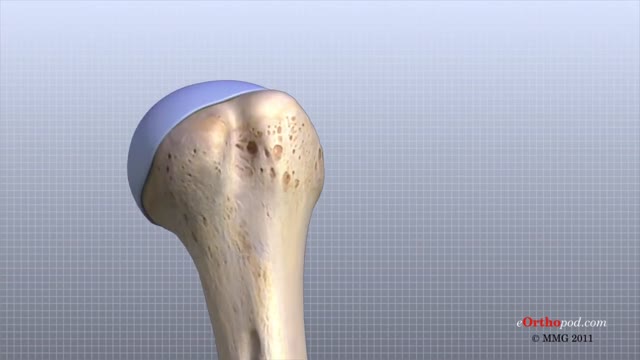
The shoulder joint is formed where the humerus (upper arm bone) fits into the scapula (shoulder blade), like a ball and socket. Other important bones in the shoulder include: The acromion is a bony projection off the scapula. The clavicle (collarbone) meets the acromion in the acromioclavicular joint.

Blood type (or blood group) is determined, in part, by the ABO blood group antigens present on red blood cells. A blood type (also called a blood group) is a classification of blood based on the presence or absence of inherited antigenic substances on the surface of red blood cells (RBCs).

An African traditional healer performing a brain surgery.

A breech birth is the birth of a baby from a breech presentation. In the breech presentation the baby enters the birth canal with the buttocks or feet first as opposed to the normal head first presentation.
There are either three or four main categories of breech births, depending upon the source:
* Frank breech - the baby's bottom comes first, and his or her legs are flexed at the hip and extended at the knees (with feet near the ears). 65-70% of breech babies are in the frank breech position.
* Complete breech - the baby's hips and knees are flexed so that the baby is sitting crosslegged, with feet beside the bottom.
* Footling breech - one or both feet come first, with the bottom at a higher position. This is rare at term but relatively common with premature fetuses.
* Kneeling breech - the baby is in a kneeling position, with one or both legs extended at the hips and flexed at the knees. This is extremely rare, and is excluded from many classifications.
As in labour with a baby in a normal head-down position, uterine contractions typically occur at regular intervals and gradually cause the cervix to become thinner and to open. In the more common breech presentations, the baby’s bottom (rather than feet or knees) is what is first to descend through the maternal pelvis and emerge from the vagina.
At the beginning of labour, the baby is generally in an oblique position, facing either the right or left side of the mother's back. As the baby's bottom is the same size in the term baby as the baby's head. Descent is thus as for the presenting fetal head and delay in descent is a cardinal sign of possible problems with the delivery of the head.
In order to begin the birth, internal rotation needs to occur. This happens when the mother's pelvic floor muscles cause the baby to turn so that it can be born with one hip directly in front of the other. At this point the baby is facing one of the mother's inner thighs. Then, the shoulders follow the same path as the hips did. At this time the baby usually turns to face the mother's back. Next occurs external rotation, which is when the shoulders emerge as the baby’s head enters the maternal pelvis. The combination of maternal muscle tone and uterine contractions cause the baby’s head to flex, chin to chest. Then the back of the baby's head emerges and finally the face.
Due to the increased pressure during labour and birth, it is normal for the baby's leading hip to be bruised and genitalia to be swollen. Babies who assumed the frank breech position in utero may continue to hold their legs in this position for some days after birth.

A chalazion is a swollen bump on the eyelid. It happens when the eyelid’s oil gland clogs up. It may start as an internal hordeolum (stye). At first, you might not know you have a chalazion as there is little or no pain. But as it grows, your eyelid may get red, swollen, and sometimes tender to touch. If the chalazion gets large, it can press on your eye and cause blurry vision. Rarely, the whole eyelid might swell.
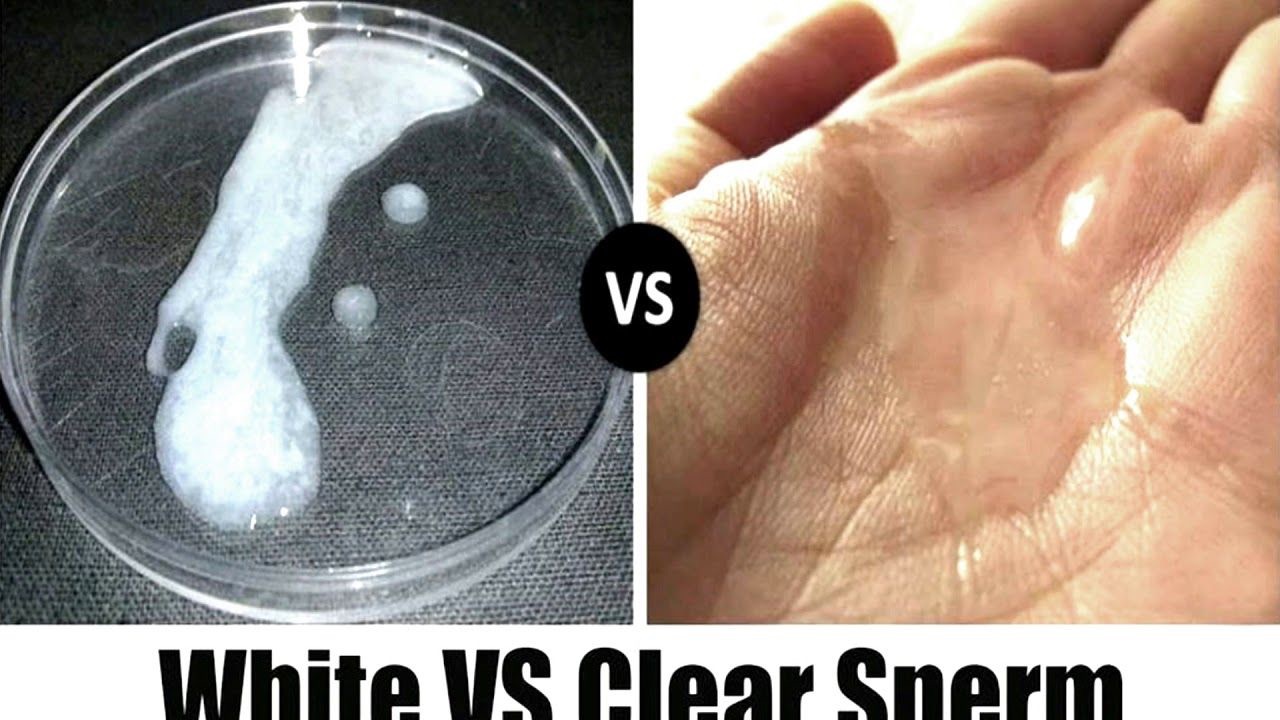
Watch that video to know the Difference Between White and Clear Sperm

Watch that Ectopic Pregnancy Medical Abortion Procedure

Watch that Full Human Dead Body Decomposing Video

The gold standard treatment for bladder outlet obstruction.This is an endoscopic procedure in which a resectoscope is placed transurethrally and the obstructing lobes of the prostate are removed as chips of tissue. TURP results in improvement of flow rate, and symptom scores are superior to that of other minimally invasive therapies
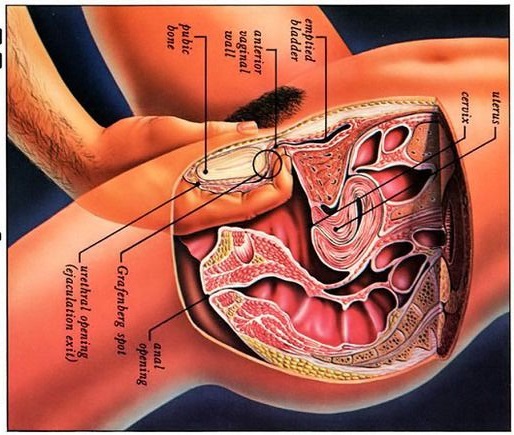
Watch that video to know what G spot is

Watch that video of Virginity Hymen Repair Plastic Surgery

For benign colorectal diseases, totally laparoscopic left-sided colectomy was already reported on some papers. Nowadays, there is increasingly demanded minimally invasive surgerys on malignant bowel diseases including colorectal cancers and so we developed the new techniques in that specimen is del...ivered through the open rectal stump, especially, using Sani Sleeve(TM). In this operation video, you can see that an anvil was fixed to proximal colonic stump with intracorporeal purse-string suture using Endo-stitch(TM). (SETA : Specimen Extraction Through Anus)
Acute Myocardial Infarction - Heart Attack

Watch that Female Foley Catheter Insertion Procedure

Clinical Examination - Gait, Arms, Legs, Spine
