- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos


Funny Video from hospital waiting room

If left untreated, these “brain blisters” can lead to stroke. Get unprecedented access inside the angiosuite to see how Babak Jahromi, MD, PhD, treats a cerebral aneurysm without ever opening the skull. #InsideTheOR
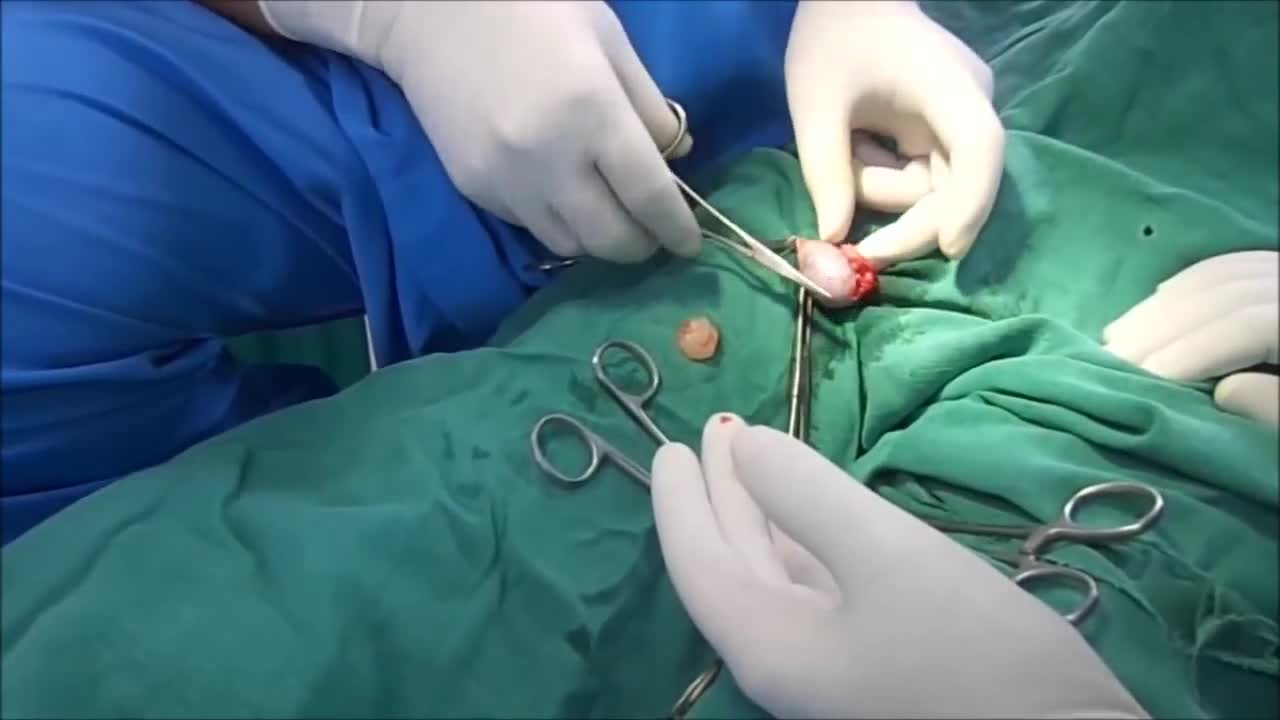
Surgery. A procedure to remove an epididymal cyst is carried out under general anaesthetic and involves removing the cysts through a small incision in your scrotum that is sealed with dissolvable stitches.

Ganglion cysts are noncancerous lumps that most commonly develop along the tendons or joints of your wrists or hands. They also may occur in the ankles and feet. Ganglion cysts are typically round or oval and are filled with a jellylike fluid. Small ganglion cysts can be pea-sized, while larger ones can be around an inch (2.5 centimeters) in diameter. Ganglion cysts can be painful if they press on a nearby nerve. Their location can sometimes interfere with joint movement. If your ganglion cyst is causing you problems, your doctor may suggest trying to drain the cyst with a needle. Removing the cyst surgically also is an option. But if you have no symptoms, no treatment is necessary. In many cases, the cysts go away on their own.

http://www.utexas.edu
Nursing students practice their skills on mannequins and each other in the Nursing Skills Lab.
Purpose: To evaluate the results of LASIK and IntraLASIK treatment in myopic patients with nystagmus. Methods: Eight patients with congenital nystagmus (16 eyes), from 23 to 49 years of age, underwent LASIK surgery. Corneal flaps were created using either the Hansatome microkeratome or the Intral...ase femtosecond laser. The ablations were performed with the Bausch & Lomb excimer laser with an active tracking system. In some patients, the eyes were fixated with forceps or a fixation ring during the laser ablation. Results: The refractive errors were corrected in all cases. There was no decentration or loss of best corrected visual acuity greater than 1 line. In 56% of the eyes, the post-operative uncorrected visual acuity was better than the best spectacle corrected-visual acuity (BSCVA). 62.5% of the eyes improved their BSCVA. The overall visual performance was improved in all the patients. One patient that did not not drive before become eligible to get a driver license after the surgery. Conclusions: Selected patients with myopia and congenital nystagmus may benefit from laser refractive surgery. Laser refractive surgery may be safely and accurately performed by using either the Hansatome microkeratome or the Intralase femtosecond laser and an active tracking system with or without mechanical fixation. Certain patients improve their BSCVA post-operatively.

Bodybuilder Drains Synthol Hematoma From Bicep

This condition is seen in imperforate hymen or transverse vaginal septum. Pt presents with primary amenorrhea. Dr Hemant Damle Prof Dept of OBGYN SKNMC Pune India
ACTUAL CATHETERIZATION A clinical view of insertion into the male urethra. A 14 french coude cath was used.

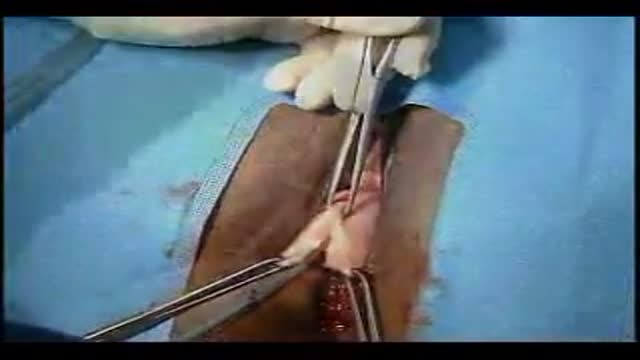
How female-to-male gender reassignment surgery works
Anterior and Posterior Vaginal Repair Plus IVS Tunne

A new video illustrating the horizontal breast exam technique whihc is performed by doctors for any breast masses or abnormalities.

Hand hygiene for healthcare workers: Learn how to perform hand washing with soap and water (nursing procedures).
There are two ways to perform hand hygiene as a nurse. You can use soap and water or an alcohol-based hand rub (also called hand sanitizer or hand gel).
Hand hygiene is essential for providing safe patient care. If hand hygiene is not performed regularly, germs can be easily be spread to patients, other healthcare workers, and even yourself.
Hand hygiene is ALWAYS performed before and after patient care, after coming into contact with any type of body fluid or open wounds, when touching any object that is near a patient (hand railing, bedside table etc.), removing gloves, prior to eating, or after using the bathroom.
This video discusses when you should use soap and water versus an alcohol-based hand gel, when to perform hand hygiene, and demonstrates how to perform hand hygiene using soap and water.
Notes: https://www.registerednursern.....com/how-to-perform-h
More nursing skills: https://www.youtube.com/watch?v=DBHnd3N-5Ns&list=PLQrdx7rRsKfUhd_qQYEbp0Eab3uUKhgKb
Facebook: https://www.facebook.com/RegisteredNurseRNs
Instagram: https://www.instagram.com/registerednursern_com/
Twitter: https://twitter.com/NursesRN
#handhygiene #handwashing #nursingskills
Subscribe: http://www.youtube.com/subscri....ption_center?add_use
Nursing School Supplies: https://www.registerednursern.....com/the-ultimate-lis
Popular Playlists:
NCLEX Reviews: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Fluid & Electrolytes: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing Skills: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing School Study Tips: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing School Tips & Questions" https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Teaching Tutorials: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Types of Nursing Specialties: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Healthcare Salary Information: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
New Nurse Tips: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Nursing Career Help: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
EKG Teaching Tutorials: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Dosage & Calculations for Nurses: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf
Diabetes Health Managment: https://www.youtube.com/playli....st?list=PLQrdx7rRsKf

Tuberous breast deformity is a congenital breast anomaly that becomes manifest at the time of puberty and breast development. The three components of tubular deformity usually include, pseudoherniation of breast tissue into the nipple areolar complex, poorly defined inframammary fold and flattening of the lower pole of the breast which leads to a conical tubular shape. Stuart Linder M.D. 9675 BRIGHTON WAY, SUITE 420 BEVERLY HILLS CA 90210 (310) 275-4513

Midline Episiotomy

Delivery using foreceps

Thanks to Ben, Addenbrooke's and neuroscientist Yaara Erez from the University of Cambridge
Anatomy of Love

General Physical Examination
