- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Furosemide is a prescription drug. It’s available in two forms that you take by mouth: a tablet and a solution. It’s also available as an injectable solution, which is given by a healthcare provider. The furosemide tablet is available as the brand-name drug Lasix. It’s also available as a generic drug. Generic drugs usually cost less. In some cases, they may not be available in every strength or form as the brand-name version.

3D Printed Models Used in the Mayo Clinic's First Face Transplant

Demonstration of Burke-Baier wound closure forceps on simulated wound near eyebrow.
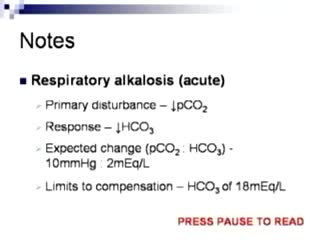
Arterial Blood Gas Sampling

Gastroschisis is a birth defect of the abdominal (belly) wall. The baby’s intestines stick outside of the baby’s body, through a hole beside the belly button. The hole can be small or large and sometimes other organs, such as the stomach and liver, can also stick outside of the baby’s body. Gastroschisis occurs early during pregnancy when the muscles that make up the baby’s abdominal wall do not form correctly. A hole occurs which allows the intestines and other organs to extend outside of the body, usually to the right side of belly button. Because the intestines are not covered in a protective sac and are exposed to the amniotic fluid, the bowel can become irritated, causing it to shorten, twist, or swell.

50 Orgasms A Day

If your knee is severely damaged by arthritis or injury, it may be hard for you to perform simple activities, such as walking or climbing stairs. You may even begin to feel pain while you are sitting or lying down. If nonsurgical treatments like medications and using walking supports are no longer helpful, you may want to consider total knee replacement surgery. Joint replacement surgery is a safe and effective procedure to relieve pain, correct leg deformity, and help you resume normal activities. Knee replacement surgery was first performed in 1968. Since then, improvements in surgical materials and techniques have greatly increased its effectiveness. Total knee replacements are one of the most successful procedures in all of medicine. According to the Agency for Healthcare Research and Quality, more than 600,000 knee replacements are performed each year in the United States. Whether you have just begun exploring treatment options or have already decided to have total knee replacement surgery, this article will help you understand more about this valuable procedure.
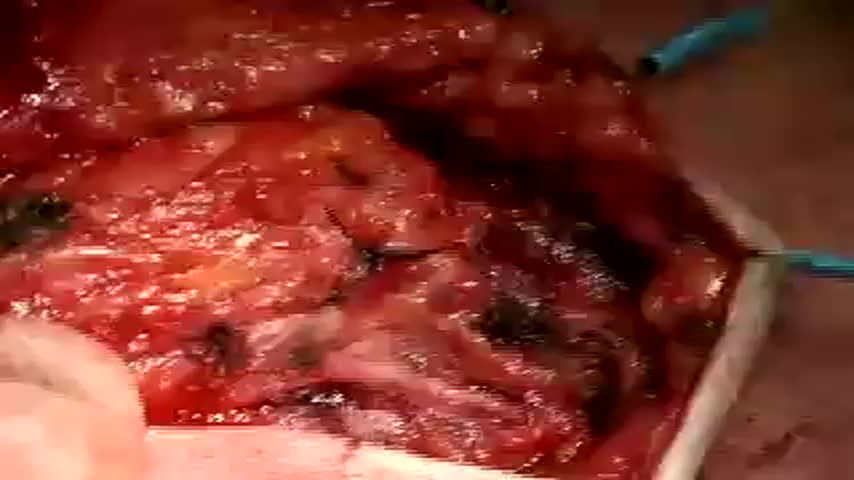
This video show the steps in a total parotidectomy with VII nerve preservation. The patient had a malignant parotid tumor without VII nerve compromise.

Frontotemporal degeneration (FTD) is a disease process that results in progressive damage to the temporal and/or frontal lobes of the brain. It causes a group of brain disorders that share many clinical features.

FemTouch Vaginal Rejuvenation Laser
Coronary artery bypass grafting (CABG) is a type of surgery that improves blood flow to the heart. Surgeons use CABG to treat people who have severe coronary heart disease (CHD). CHD is a disease in which a waxy substance called plaque (plak) builds up inside the coronary arteries.
Watch that video to know if it is safe to have anal sex
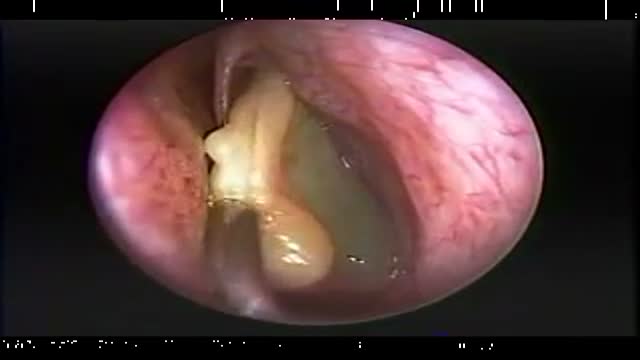
Endoscopic Nasal Polypectomy

http://penilepapules.plus101.com/ ----- White Spots On Shaft, Pearly Penile Papules Treatment Cream, Single Red Bump On Shaft, Ppp Surgery. Common Home Made Remedies for Pearly Penile Papules. When it comes to treating pearly penile papules many people find it very difficult to reach one of the medical treatments. This is mainly because they are highly expensive and not many people can afford spending large amounts of money on surgery and recovery. In addition to that, these procedures have been reported as being quite risky, which make the men suffering from pearly penile papules think twice before going for one of the available surgeries. This is why, along the time, many homemade, natural treatments have been experienced, so that a cheaper and less risky way of curing pearly penile papules would be found. Some of the methods which have been tried proved to be very less effective, while some did not have any effect at all. Yet, there have also been methods which not only proved to be effective, but they were also considered to be much better than the medical treatment. Most of those who have tried the tea tree oil treatment reported significant diminish of the number of the papules from their penises. In addition to the clearing of the skin, they have also noticed that there were no side effects and the skin remained soft after the papules were removed. As the method was quite simple to put in practice (it requires the application of tea tree oil on the affected area with a cotton swab for three or four times per day), many men decided this was indeed a great solution to their problem.
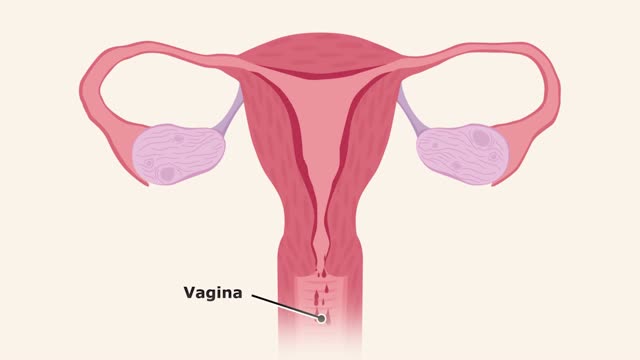
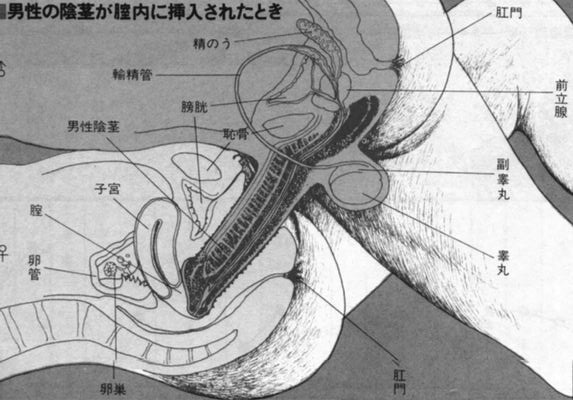
The menstrual cycle is the monthly series of changes a woman's body goes through in preparation for the possibility of pregnancy. Each month, one of the ovaries releases an egg — a process called ovulation. At the same time, hormonal changes prepare the uterus for pregnancy.

Curettage, electrosurgery, and laser surgery are more likely than cryotherapy to leave scars, so they are usually reserved for hard-to-remove or recurring warts. If you have a large area of warts, curettage may not be an effective treatment. Some surgical treatments may be too painful for some children.
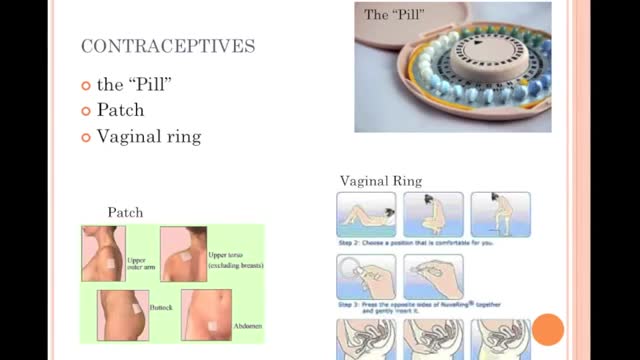
Choosing not to have sex provides 100 percent protection from HIV, STIs, and pregnancy. For some, this means avoiding vaginal, anal, and oral-genital intercourse altogether. Others may choose to avoid any type of sexual or intimate contact, including hugging and kissing. Choosing not to have sex is often referred to as “abstinence.” WHAT ARE THE ADVANTAGES OF CHOOSING NOT TO HAVE SEX (ABSTINENCE)? Choosing not to have sex is free and available to all. Not having sex is extremely effective at preventing both infection and pregnancy. It is the only 100% effective method of preventing sexually transmitted infections (STIs) and unintended pregnancy. Not having sex can be practiced at any time in one's life. Not having sex may encourage people to build relationships in other ways. Not having sex may be the course of action which you feel is right for you and makes you feel good about yourself.
Acute bronchitis and pneumonia share many of the same symptoms, and some people with acute bronchitis are at risk for getting pneumonia. Although acute bronchitis usually goes away within a few weeks, pneumonia can be a serious condition, especially in older adults. The following table outlines some differences between acute bronchitis and pneumonia. There are variations in symptoms of both conditions, so if you think you might have pneumonia, always check with your doctor.

http://barretts-esophagus-cure.info-pro.co Barrett's Esophagus, Barrett's Esophagus Metaplasia, Barrett's Esophagus Bulimia. Are you lost, scared, frustrated, or confused? Have you been recently diagnosed with Barrett’s? Maybe your loved one or a close family member is now a victim of this painful disease. If so, I’d like to share with you some possibly life changing information on how I personally cured my own Barrett’s Esophagus. But before I do I’d like you to take a deep breath, relax for a moment, and let your worry subside because. Even though the Society of Thoracic Surgeons has determined that people with Barrett’s Esophagus are 40x’s more likely to get esophageal cancer, this diagnosis isn’t always a death sentence. Having been a victim of Barrett’s myself, I can relate to the excruciating pain this disease can cause. Maybe you’re like I was, trying to hide the symptoms when the burning, the heartburn, and the PAIN would become so unbearable I’d try doing anything to block it out. I can clearly recall the feeling of those scorching corroding acids inside my throat that would burn like fire, tearing up my esophagus from the inside out. It’s a pain I will NEVER forget. For me, maybe like you, many of my days were spent in anguish and painful agony. Barrett’s Reversed Without Surgery, Pills, PPI Pumps, Antacids, or Drugs. Clicking Here http://barretts-esophagus-cure.info-pro.co

A usage instruction on how to use a female condom (also know as a Femidom). Female Condom Application and Removal.
