- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Beta-blockers, also known as beta antagonists, beta-adrenergic blocking agents, or beta-adrenergic antagonists, are drugs that are prescribed to treat several different types of conditions, including hypertension (high blood pressure), angina, some abnormal heart rhythms, heart attack (myocardial infarction), anxiety, migraine, glaucoma, and overactive thyroid symptoms.
Menorrhagia is the medical term for menstrual periods with abnormally heavy or prolonged bleeding. Although heavy menstrual bleeding is a common concern, most women don't experience blood loss severe enough to be defined as menorrhagia. With menorrhagia, you can't maintain your usual activities when you have your period because you have so much blood loss and cramping. If you dread your period because you have such heavy menstrual bleeding, talk with your doctor. There are many effective treatments for menorrhagia. Symptoms Signs and symptoms of menorrhagia may include: Soaking through one or more sanitary pads or tampons every hour for several consecutive hours Needing to use double sanitary protection to control your menstrual flow Needing to wake up to change sanitary protection during the night Bleeding for longer than a week Passing blood clots larger than a quarter Restricting daily activities due to heavy menstrual flow Symptoms of anemia, such as tiredness, fatigue or shortness of breath


Acanthosis Nigricans Insulin Resistance
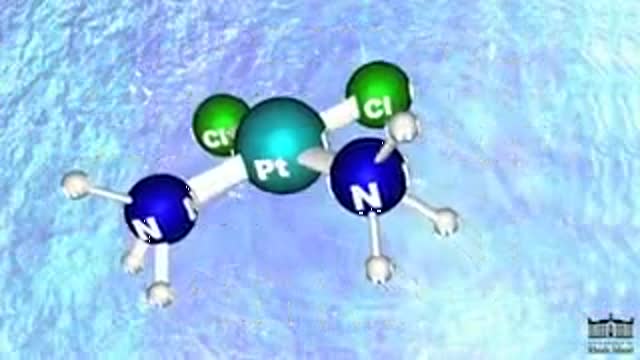
Cisplatin is in a class of drugs known as platinum-containing compounds used to treat various types of cancers including metastatic testicular and ovarian tumors. The molecule was first discovered in 1845, but did not receive FDA approval until 1978. Today it is known as the "penicillin of cancer drugs," because it is so effective for many different cancers. There are three key players involved in Cisplatin's mechanism: (1) Cisplatin, (2) DNA (3) and an HMG Protein. Most Cisplatin enters the body through active transport, but some molecules are passively defused through the cell membrane. Once in the nucleus, Cisplatin can form an adduct with two consecutive guanine bases within a strand of DNA. The molecule loses its chlorine atoms in exchange for the nitrogen atoms of the target guanines. Cisplatin can bond more tightly with nitrogen because nitrogen balances the platinum charge more effectively than chlorine. It is this adduct-induced DNA bend that allows binding of proteins which contain the high mobility group, HMG domain. Once the protein is bound to the DNA, it inserts a wedge-like phenyl group of phenylalanine 37 into the widened minor groove created by the bend. The tightly bound HMG protein causes destacking of the nucleotide bases, resulting in the DNA helix becoming kinked. In this way, Cisplatin can be thought of as a monkey wrench in the DNA repair system. With the HMG protein bound to the DNA, the modified strand is not repaired properly and so the cell dies. The success of Cisplatin depends on its ratio of efficacy between cancerous and healthy cells.
USMLE Step 2 CS - Diabetes Mellitus This is just preview video. To get full access please visit our website : www.usmletutoring.com
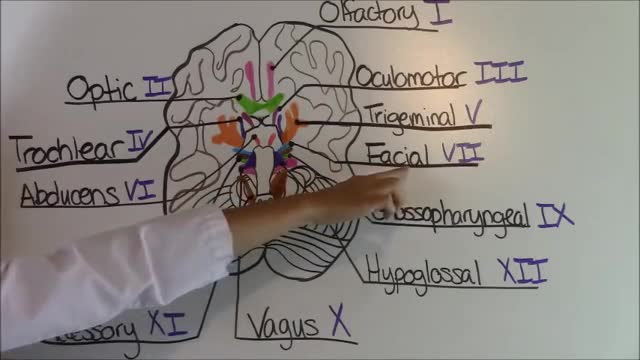
Cranial Nerves Mnemonic


Learn all about the differences between these important hernias!

Blood cells travel through the circulatory system suspended in a yellowish fluid called plasma. Plasma is 90% water and contains nutrients, proteins, hormones, and waste products. Whole blood is a mixture of blood cells and plasma.

Pediatric febrile seizures, which represent the most common childhood seizure disorder, exist only in association with an elevated temperature. Evidence suggests, however, that they have little connection with cognitive function, so the prognosis for normal neurologic function is excellent in children with febrile seizures. [1] Epidemiologic studies have led to the division of febrile seizures into 3 groups, as follows: Simple febrile seizures Complex febrile seizures Symptomatic febrile seizures Essential update: Starting MMR/MMRV vaccination earlier may reduce seizure risk In a case-series analysis of a cohort of 323,247 US children born from 2004 to 2008, Hambidge et al found that delaying the first dose of measles-mumps-rubella (MMR) or measles-mumps-rubella-varicella (MMRV) vaccine beyond the age of 15 months may more than double the risk of postvaccination seizures in the second year of life. [2, 3] In infants, there was no association between vaccination timing and postvaccination seizures. [3] In the second year of life, however, the incident rate ratio (IRR) for seizures within 7-10 days was 2.65 (95% confidence interval [CI], 1.99-3.55) after first MMR doses at 12-15 months of age, compared with 6.53 (95% CI, 3.15-13.53) after first MMR doses at 16-23 months. For the MMRV vaccine, the IRR for seizures was 4.95 (95% CI, 3.68-6.66) after first doses at 12-15 months, compared with 9.80 (95% CI, 4.35-22.06) for first doses at 16-23 months.
Male Foley Catheterization Technique

After the diagnosis of primary melanoma of pectoral region had been established, the patient was referred to lymphoscintigraphy with gamma camera (techencium; nanno colloid). Two hours after the administration of the contrast medium, the operation commenced. During the operation the primary tumor wa...s excised, and the sentinel node was detected with the use of gamma probe and also excised.


SEX DURING PREGNANCY & 7 Tips For A Healthy Pregnancy
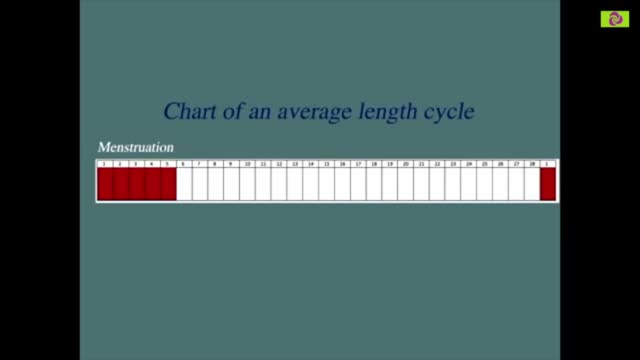
Our calculator can help you discover the most fertile days of your menstrual cycle or your “Estimated Fertility Window” based on information you provide.

Enchondroma (Cartilage) benign tumor of the finger.
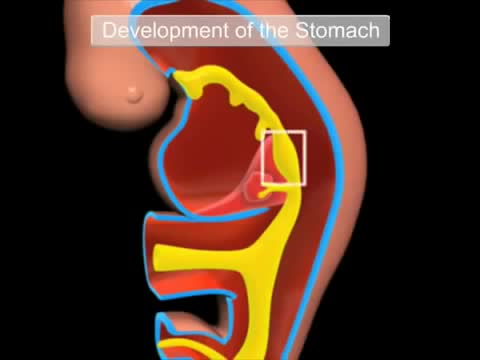
The gastrointestinal tract (GIT) arises initially during the process of gastrulation from the endoderm of the trilaminar embryo (week 3) and extends from the buccopharyngeal membrane to the cloacal membrane. The tract and associated organs later have contributions from all the germ cell layers. During the 4th week three distinct regions (fore-, mid- and hind-gut) extend the length of the embryo and will contribute different components of the GIT. The large mid-gut is generated by lateral embryonic folding which "pinches off" a pocket of the yolk sac, the 2 compartments continue to communicate through the vitelline duct. The oral cavity (mouth) is formed following breakdown of the buccopharyngeal membrane (oropharyngeal or oral membrane) and contributed to mainly by the pharynx lying within the pharyngeal arches (More? Head Development). Loss of buccopharyngeal membrane opens the tract to amniotic fluid through the remainder of development, and during the fetal period is actively swallowed.

McMaster University technique of Laparoscopic Radical Nephrectomy
