- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
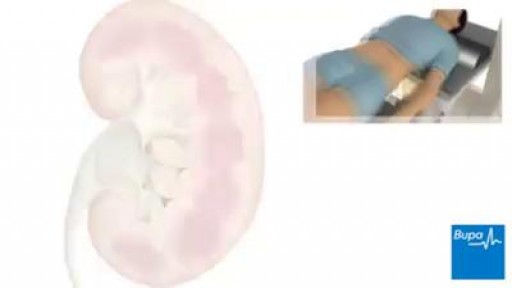
extracorporeal shockwave lithotripsy is used to treat kidney stones

Welcome to the latest episode of HT Physio Quick Tips!
In this episode, Farnham's leading over-50's physiotherapist, Will Harlow, reveals the THREE most serious knee injuries and gives the signs and symptoms that indicate a serious knee injury has occurred.
To get a copy of Will's new book, Thriving Beyond Fifty, you can visit here: https://www.amazon.co.uk/Thriv....ing-Beyond-Fifty-Str
If you're suffering from nagging knee pain that hurts in the morning and stops you from walking as far as you'd like, you can take our free knee pain guide - which will give you 5 expert tips to put a stop to knee pain at home - by visiting here: https://ht-physio.co.uk/knee-pain-guide-download/
If you're over-50 with a painful problem in the Farnham, Surrey area, you can learn more about how Will Harlow and HT Physio can help you overcome a painful problem here: https://ht-physio.co.uk/
**Any information in this video should not be used as a substitute for individual medical advice. Please seek advice from your local healthcare professional before taking action on the information in this video.**

After Sammyra’s knee injury, Marvin Smith, MD, orthopaedic surgeon at Memorial Sports Medicine Center, helped her get back on the volleyball court and playing pain free. Following a thorough examination, meniscus surgery and rehabilitation got Sammyra back to playing with her college team within two months. Learn more about how Memorial Sports Medicine Center helps athletes move forward at MHS.net/SportsMedicine.
To learn more about Dr. Smith, visit his physician profile page at: https://www.mhs.net/physicians/s/smith-marvin-k

Straight Leg Raising from the USMLE collection
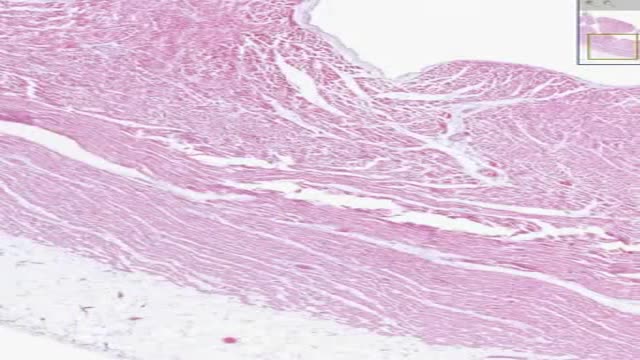
Histology of Heart Cardiac Muscle

fixation of a tibial fracture utilizing the Titanium Cannulated Tibial Nail
Providing information on the Atherosclerosis and its complex biological process: it is the idea of this medical video dedicated to the prevention of the cardiovascular risks of diseases.
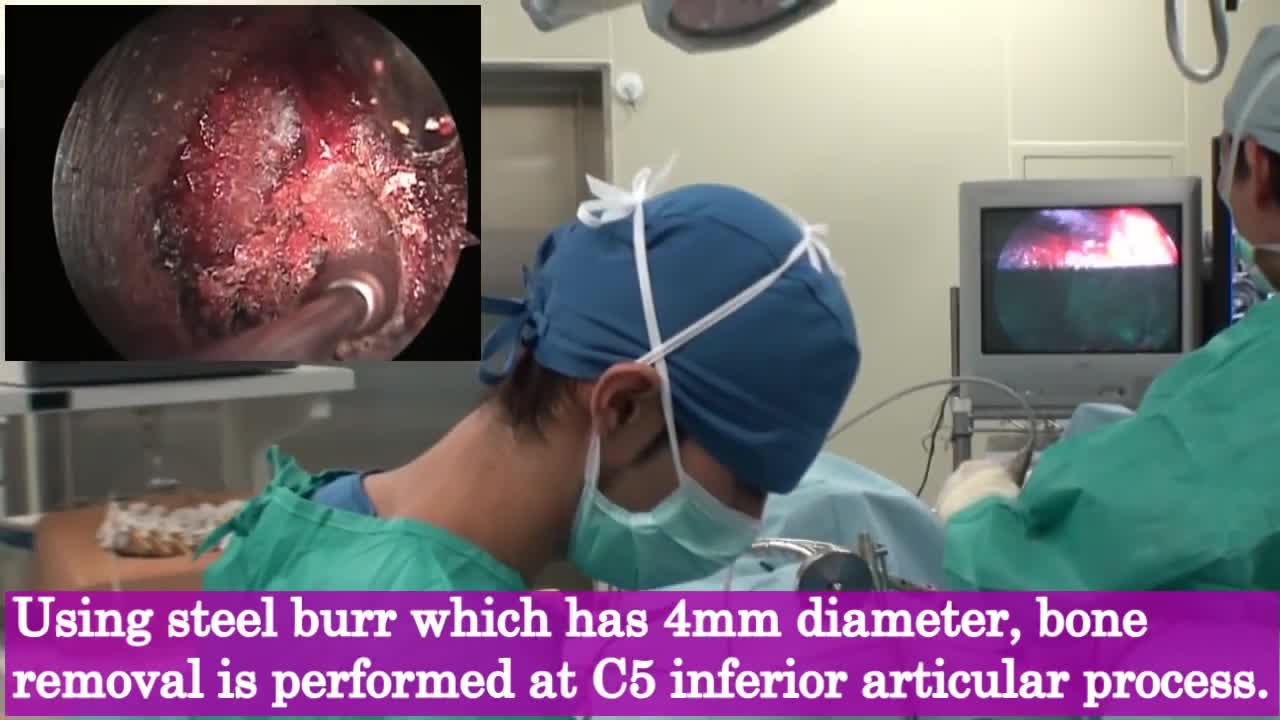
A cervical herniated disc may be treated by removing part of the disc through a small incision (microdiscectomy). If this is done from the back (posteriorly) rather than from the front of the neck, a spinal fusion is not necessary. The alternative is an anterior cervical discectomy and fusion procedure.

Spina bifida is a type of birth defect called a neural tube defect. It occurs when the bones of the spine (vertebrae) don't form properly around part of the baby's spinal cord. Spina bifida can be mild or severe. The mild form is the most common.

Ruth’s testimonial on her amazing experience with cosmetic dental procedures offered by Dr Jamil Alkhoury at Brentwood Family Dental

Special Anoscope for Easy Purse string Suture Application in Stapled Hemorrhoidopexy
Spinal stenosis can put pressure on the spinal cord and the nerves within the spine. It commonly occurs in the neck and lower back. The condition is often caused by age-related wear and tear. Symptoms, if they occur, include pain, numbness, muscle weakness, and impaired bladder or bowel control. Treatment includes medication, physical therapy, and possibly surgery

The abortion pill is a medicine called mifepristone that ends an early pregnancy.In general, it's used up to 70 days — 10 weeks — after the first day of a woman's last period. Patients over this mark can have an in-clinic abortion procedure.
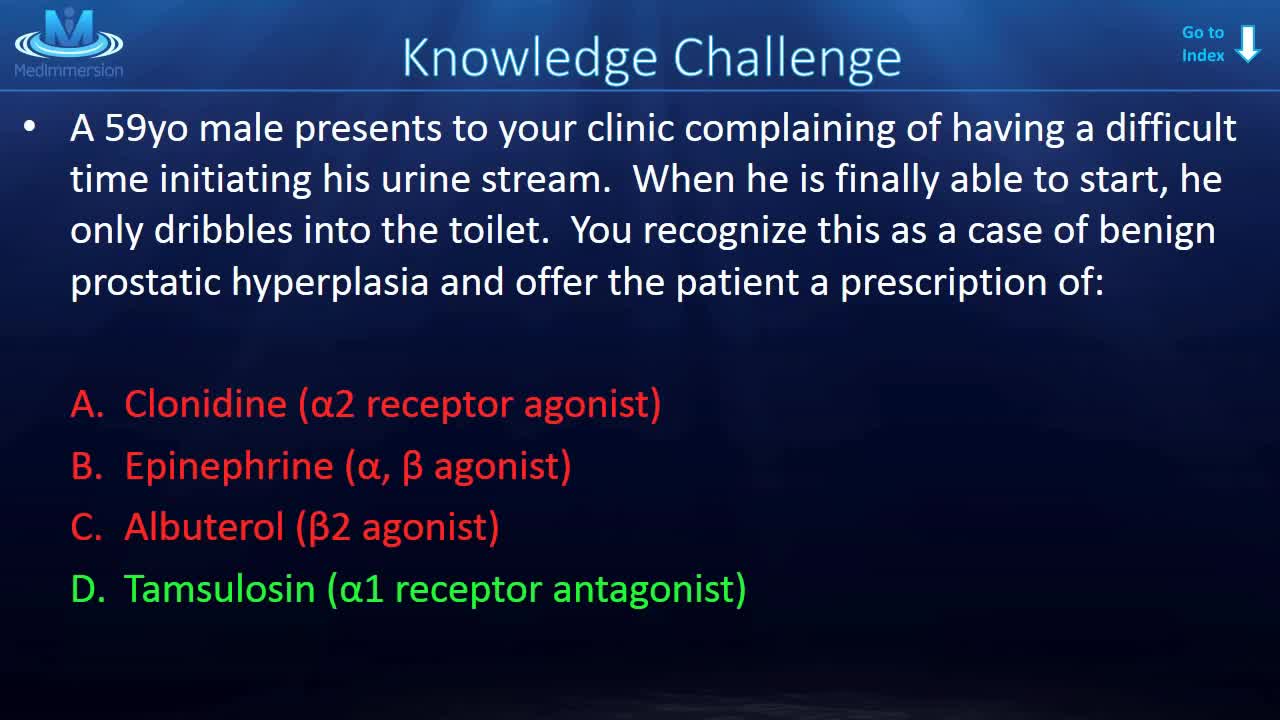
Understanding the adrenergic receptors is fundamental to a solid grasp of adrenergic pharmacology!

A video showing impaled objects

How a simple conversation about colon cancer screening can save your life.

Preventing Hemodialysis Catheters Problems

دكتور مصطفى ياقوت فى حوار على القناة الفضائية المصرية عن الطب البديل و الطب الفرعونى فى علاج الأرق
TV interview with Dr. Mostafa Yakoot about Alternative medicine
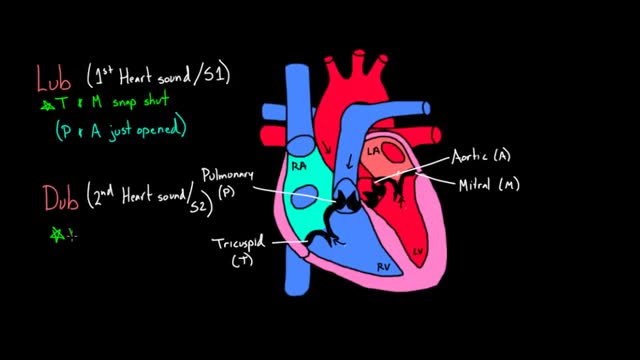
The heart and circulatory system (also called the cardiovascular system) make up the network that delivers blood to the body's tissues. With each heartbeat, blood is sent throughout our bodies, carrying oxygen and nutrients to all of our cells.
