- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Physical Examination Introduction

A c-section, or cesarean section, is the delivery of a baby through a surgical incision in the mother's abdomen and uterus. In some circumstances, a c-section is scheduled in advance. In others, the surgery is needed due to an unforeseen complication. If you or your baby is in imminent danger, you'll have an emergency c-section. Otherwise, it's called an unplanned section. According to the U.S. Centers for Disease Control, about 32 percent of American women who gave birth in 2015 had a cesarean delivery.
Dr. Katherine Scovner from the Division of Nephrology at Massachusetts General Hospital discusses kidney dialysis.

A VCUG (Voiding Cystourethrogram) is a test that looks at how well your child's kidneys, ureters and bladder are working. Your child's kidneys make urine. The urine flows from the kidneys through thin tubes (called ureters) into your child's bladder.

Watch that Female Body Medical Autopsy for Anatomy Class

On this week's episode of Macro Beauty, we follow a young woman on her journey to getting Lasik eye surgery. She opts for this corrective vision procedure and we captured it up close. Watch this video to see what the process is really like!
https://maloneyvision.com/
ABOUT SERIES
We're getting up close and personal into all things beauty. Have you ever wondered whether or not waterproof mascara really works? Or been intrigued with tattooing your eyebrows? We'll show you this process like you have never seen it before!
ABOUT REFINERY29
Refinery29 is a modern woman's destination for how to live a stylish, well-rounded life. http://refinery29.com/
RELATED CONTENT
Why I Got This 15 Minute Nose Job
https://youtube.com/watch?v=_TGq8Uuvf0w
Microblading Permanent Eyebrow Tattoo Up Close
https://youtube.com/watch?v=HhdTcySV9zo
How To Get A Nose Piercing With Brian Keith Thompson Of Body Electric
https://youtube.com/watch?v=OPhvc_4kjas
SEE MORE REFINERY29 VIDEOS
http://refinery29.com/video
SUBSCRIBE TO REFINERY29
Subscribe to the Refinery29 channel: http://bit.ly/subscribe-to-r29
For the latest trends and videos, visit: http://refinery29.com
Like Refinery29 on Facebook: https://facebook.com/refinery29
Follow Refinery29 on Twitter: https://twitter.com/refinery29
Heart Refinery29 on Instagram: https://instagram.com/refinery29/
TALENT
Follow The Maloney Shamie Vision Institute on Instagram: https://instagram.com/maloneyvision/
Follow Emily on Instagram: https://instagram.com/emmy_free/
Follow Unbothered on Instagram: https://instagram.com/r29unbothered/
Follow OnHerTurf on Instagram: https://instagram.com/onherturf/
Follow Refinery29 on Instagram: https://instagram.com/refinery29/

Foley Catheter Insertion
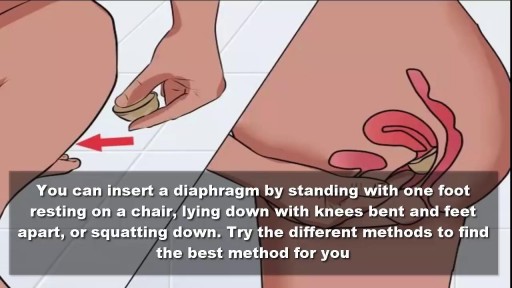
To use the diaphragm, first cover the inside of it with spermicide. Then insert it into your vagina so that it covers your cervix. You can insert the diaphragm up to 6 hours before sex. You should leave it in for at least 6 hours after the last time you have sex.

A bone-anchored hearing aid (BAHA) or bone-anchored hearing device,is a type of hearing aid based on bone conduction. It is primarily suited for people who have conductive hearing losses, unilateral hearing loss, single-sided deafness and people with mixed hearing losses who cannot otherwise wear 'in the ear' or 'behind the ear' hearing aids. They are more expensive than conventional hearing aids, and their placement involves invasive surgery which carries a risk of complications, although when complications do occur, they are usually minor. Two of the causes of hearing loss are lack of function in the inner ear(cochlea) and when the sound has problems in reaching the nerve cells of the inner ear. Example of the first include age-related hearing loss and hearing loss due to noise exposure. A patient born without external ear canals is an example of the latter for which a conventional hearing aid with a mould in the ear canal opening would not be effective. Some with this condition have normal inner ear function, as the external ear canal and the inner ear are developed at different stages during pregnancy. With normal inner anatomy, sound conducted by the skull bone improves hearing.
A video showing the repair of episiotomy

No two people alike. Here are the 10 most rare and strange medical conditions all expecting parents dread.

Join the Amoeba Sisters a they explore different muscle tissues and then focus on the sliding filament theory in skeletal muscle! This video also briefly talks about muscle naming, some vocabulary (such as agonists and antagonists) before focusing on the sliding filament model. Video also mentions general roles of tropomyosin and troponin.
---------------------------------------------------------
Table of Contents:
00:00 Intro
0:39 Muscle Tissue Types
1:58 Muscle Characteristics
2:33 Skeletal Muscle Naming and Arrangement
3:26 Actin Myosin and Sarcomere
4:32 Sliding Filament Model
6:55 Tropomyosin an Troponin
---------------------------------------------------------
Factual References:
Betts, J. Gordon, et al. “10.3 Muscle Fiber Contraction and Relaxation - Anatomy and Physiology 2e | OpenStax.” Openstax.org, 20 Apr. 2022, openstax.org/books/anatomy-and-physiology-2e/pages/10-3-muscle-fiber-contraction-and-relaxation.
Urry, Lisa A, et al. Campbell Biology. 11th ed., New York, Ny, Pearson Education, Inc, 2017.
---------------------------------------------------------
Further Reading Recommendations:
What about I and A bands? What actually initiates the power stroke? How does calcium get released and from where? Remember, there is a lot more detail! We recommend this page from Openstax to learn more:
https://openstax.org/books/bio....logy-2e/pages/38-4-m
-----------------------------------------------
The Amoeba Sisters videos demystify science with humor and relevance. The videos center on Pinky's certification and experience in teaching biology at the high school level. Amoeba Sisters videos only cover concepts that Pinky is certified to teach, and they focus on her specialty: secondary life science. Learn more about our videos here: https://www.amoebasisters.com/our-videos
Support Us? https://www.amoebasisters.com/support-us
Our Resources and Handouts: https://www.amoebasisters.com/handouts
Biology Video Playlist: https://www.youtube.com/playli....st?list=PLwL0Myd7Dk1
GIFs: https://www.amoebasisters.com/gifs.html
Comics: https://www.amoebasisters.com/....parameciumparlorcomi
Unlectured Series: https://www.amoebasisters.com/unlectured
Connect with us!
Website: https://www.AmoebaSisters.com
Twitter: https://www.twitter.com/AmoebaSisters
Facebook: https://www.facebook.com/AmoebaSisters
Tumblr: https://www.amoebasisters.tumblr.com
Pinterest: https://www.pinterest.com/AmoebaSisters
Webtoon: https://www.webtoons.com/en/challenge/amoeba-sisters-sisterhood/list?title_no=289479&page=1
Instagram: https://www.instagram.com/amoebasistersofficial/
TikTok: https://www.tiktok.com/@amoebasistersofficial
Visit our Redbubble store at https://www.amoebasisters.com/store
TIPS FOR VIEWING EDU YOUTUBE VIDEOS:
Want to learn tips for viewing edu YouTube videos including changing the speed, language, viewing the transcript, etc? https://www.amoebasisters.com/....pinkys-ed-tech-favor
MUSIC:
Our intro music designed and performed by Jeremiah Cheshire.
End music in this video is listed free to use/no attribution required from the YouTube audio library.
COMMUNITY:
We take pride in our AWESOME community, and we welcome feedback and discussion. However, please remember that this is an education channel. See YouTube's community guidelines and how YouTube handles comments that are reported by the community. We also reserve the right to remove comments.
TRANSLATIONS:
Spanish Subtitles Translated by Jeremy García
Hindi Subtitles: Translated by Alisha Aggarwal
We gladly accept subtitle translations from our community. Learn more here: https://www.amoebasisters.com/....pinkys-ed-tech-favor We want to thank our amazing community for the generosity of their time in continuing to create translated subtitles.
We also have videos dubbed in Spanish and Portuguese using an artificial voice via https://aloud.area120.google.com to increase accessibility. See our Amoeba Sisters en Español channel https://www.youtube.com/channe....l/UC1Njo3LBy53cOPngz and Amoeba Sisters em Português https://www.youtube.com/channe....l/UCYTQPX2X_mXe0ZMPi

Watch that video of Sperm Formation and Ejaculation Process

Brain port surgery is a minimally invasive surgical technique performed through a specially designed tube about the size of a dime. Using neuronavigation GPS-like guidance, the brain port is inserted into the brain with millimeter accuracy and is used as a channel to guide the surgeon and his/her instruments to various regions of the brain. Colloid cysts, metastatic tumors, and a variety of tumors within the ventricles are often candidates for this approach.

Traditional Chinese fire cupping therapy
Understand how this world-class surgery platform operates a minimally invasive robotic surgery during a medical procedure for prostate cancer.

Many U.S. hospitals still perform traditional surgery, over minimally invasive procedures, according to Johns Hopkins University researchers. Also, a new study on HPV vaccines. Wendy Gillette reports on the day's top health stories.


Full Tummy Tuck 3D Video - http://drlandsman.com
Look great... feel great
•Smart Liposuction + Liposculpture
•Abdominplasty (Tummy Tuck)
+ Full Mini Modified
•Brazilian Lift with Fat Transfer
•Vaginal Aesthetics & Rejuvenation
•Laser Hair Removal
•Full Body Lift
•Thigh lift
•Brachioplasty (Arm Lift) + Short Scar
Expertise in Body Contouring
Board Certified Plastic Surgeon
Expertise in body contouring combines skin excision techniques and advanced fat contouring technology
Weight control personalized training and smoking cessation results in a healthier lifestyle improved shape and longer lasting results
With over 2 decades of experience Dr Lloyd Landsman provides state of the art cosmetic and plastic surgery
Dr Landsman integrates the finest and safest products with the newest procedures
A customized treatment plan is created for each patient utilizing classic surgical and minimally invasive techniques for optimal results
Call for your complimentary consultation to learn how Dr Landsman can help you look your very best
Visit http://drlandsman.com Call 631 864 4111
Main Office 994 W Jericho Tpke Smithtown NY 11787
Affiliates East Islip • Westbury • Jackson Heights • Manhattan
