- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos


An Abdominoplasty (commonly referred to as a “Tummy Tuck”) removes excess fat and skin around your abdomen to shape and contour your midsection. During surgery, I also restore weakened or separated muscles to help create an abdominal profile that is both; smoother and more firm.
Watch this video as we go from the operating table to her 2-month post-op results!
If you’re interested in learning more about tummy tuck surgery or any other services we offer, please DM us or give us a call today!
☎️(424) 266-4181
🌐DrJohnDiaz.com
#DrJohnDiaz #DrDiaz #BeverlyHills #BeverlyHillsPlasticSurgery #BeverlyHillsPlasticSurgeon #DiazPlasticSurgery #PlasticSurgery #PlasticSurgeon #TummyTuck #Abdominoplasty #BeverlyHillsTummyTuck #TummyTuckBeverlyHills #AbdominoplastyBeverlyHills #BeverlyHillsAbdominoplasty #TummyTuckSurgery
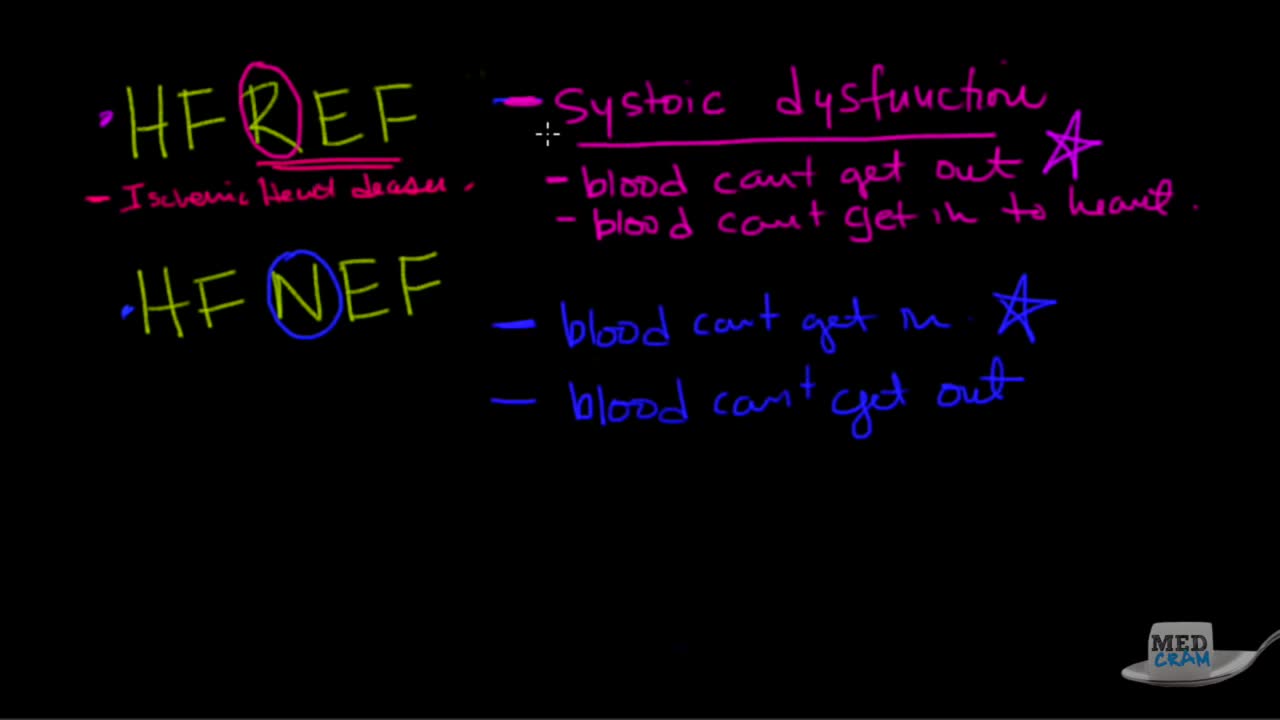
Heart failure, sometimes known as congestive heart failure, occurs when your heart muscle doesn't pump blood as well as it should. Certain conditions, such as narrowed arteries in your heart (coronary artery disease) or high blood pressure, gradually leave your heart too weak or stiff to fill and pump efficiently.

DMC Neurosurgeon Sandeep Mittal maps the brain and performs delicate surgery to remove epileptic tissue, and stop a patient's seizures. ~ Detroit Medical Center

A man's age matters. As men get older, the chances of conceiving and having a healthy child decline. Male fertility starts to decline after 40 when sperm quality decreases. This means it takes longer for their partners to conceive and when they do, there's an increased risk of miscarriage.
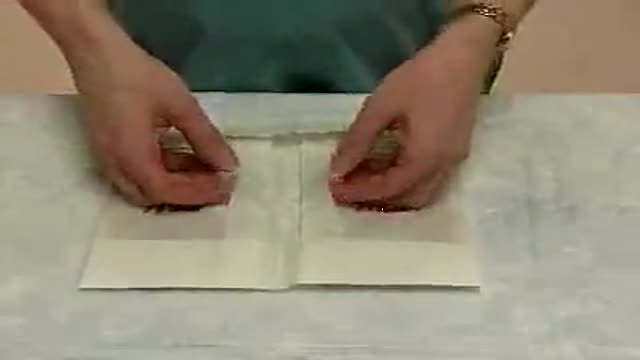
How to put on sterile gloves using aseptic technique.


Hepatitis B is a serious liver infection caused by the hepatitis B virus (HBV). For some people, hepatitis B infection becomes chronic, meaning it lasts more than six months. Having chronic hepatitis B increases your risk of developing liver failure, liver cancer or cirrhosis — a condition that causes permanent scarring of the liver. Most people infected with hepatitis B as adults recover fully, even if their signs and symptoms are severe. Infants and children are more likely to develop a chronic hepatitis B infection. A vaccine can prevent hepatitis B, but there's no cure if you have it. If you're infected, taking certain precautions can help prevent spreading HBV to others.

Nursing skills lab procedure for IV insertion.

Endoscopic finding in a patient with a typical rectal cancer (adenocarcinoma)

Each year in the United States, about 400 children and teens younger than age 20 are diagnosed. Osteosarcoma is the third most common cancer in teens, after lymphomas and brain tumors. It is extremely rare in children before age 5.
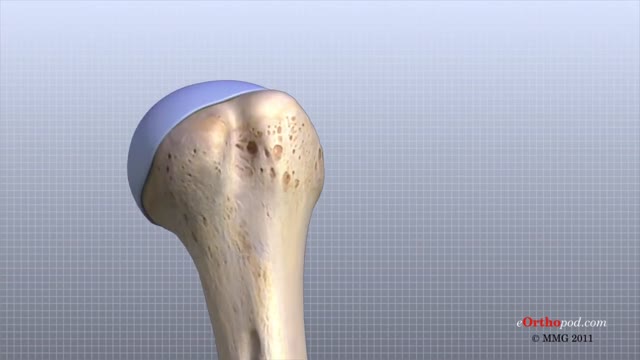
The shoulder joint is formed where the humerus (upper arm bone) fits into the scapula (shoulder blade), like a ball and socket. Other important bones in the shoulder include: The acromion is a bony projection off the scapula. The clavicle (collarbone) meets the acromion in the acromioclavicular joint.

1. What is hemodialysis?
2. Why do you do hemodialysis?
3. How does hemodialysis remove body waste?
4. What are the symptoms and side effects of hemodialysis?
5. How should I eat food when I do hemodialysis?
6. What are some precautions for patients during hemodialysis?
► If you have any health issues contact us anytime, we here to help at CloudHospital – https://icloudhospital.com/
► Subscribe: https://www.youtube.com/channel/UCmk5... to learn more about various health and beauty topics.
► Find us on Facebook: https://www.facebook.com/icloudhospital/
► On Instagram: https://www.instagram.com/cloudhospit...
► On LinkedIn: https://www.linkedin.com/company/clou...
► On Twitter: https://twitter.com/CloudhospitalI
#hemodialysis #cloudhospital #koreahospital
![What does a fistula for dialysis look like? [CHT CERTIFICATION REVIEW] 2022](https://i.ytimg.com/vi/gjB5eKo4eh8/maxresdefault.jpg)
If this is the first time visiting us, make sure to subscribe to our channel here: https://bit.ly/2yXNBYp
What does a fistula for dialysis look like?
A fistula for dialysis is a surgical connection between a vein and an artery.
In this video, I will show you a real fistula and how we should evaluate it before a dialysis connection.
Additional videos:
💉How to properly cannulate a fistula: https://youtu.be/IqoHnzFyhJQ
💉 What is a fistula for dialysis treatment: https://youtu.be/B5EEf-MklFk
💉 The 10-second assessment for fistulas: https://youtu.be/Uqo0LhjZSI8
💉 If you would like to be trained as a dialysis professional focused on offering quality of care to renal patients, visit our program details here: https://utopiahcc.com/hemodialysis-technician/
For nursing and technician schools😷 🩺 🎓, we can offer a special renal failure class to your students. For inquiries please contact us: info@utopiahcc.com
Where to find us:
Facebook: https://www.facebook.com/utopiahealth
Email: info@utopiahcc.com
Website: utopiahcc.com
🤔 Looking for renal and dialysis continuing education for your certification renewal? Check out our CE package where you will get a little over 40 contact hours for a small price and receive your certificates immediately.
Here's the link: https://bit.ly/3dbPvDZ
Want to watch *Free Dialysis Training Videos*?
https://utopiahcc.com/free-dia....lysis-video-training
__________________________________________________________
Additional resources:
What Does a Healthy AV Fistula Look Like? | Azura Vascular ...
www.azuravascularcare.com infodialysisaccess healt...
Jul 17, 2018 — An AV fistula is a surgically-created permanent access located under the skin, making a direct connection between a vein and an artery. An AV fistula is typically created in the non-dominant arm. If the veins in your arm are not large or healthy enough to support a fistula, it may be created in your leg.
Preparing for Dialysis (AV Fistula) Fact Sheets Yale ...
www.yalemedicine.org › conditions › preparing-dialysi...
To undergo dialysis, patients need a surgical procedure to create an access point for the dialysis machine. An AV fistula is the most common access point.
Vascular Access for Hemodialysis - Life Options
lifeoptions.org living-with-kidney-failure vascular-a...
Jump to How a Catheter Looks and Feels — This makes a pattern that looks a bit like a rope ladder. The next best way—for fistulas ONLY—is the “Buttonhole ...
Fistula or Graft Surgery · Needle Fear · How a Fistula or Graft Looks...
Taking Care of Your Fistula - DaVita
www.davita.com dialysis preparing-for-dialysis › ta...
An arteriovenous (AV) fistula is a type of access used for hemodialysis. ... access because it utilizes the patient's own vessels and does not require permanent placement of foreign materials such ... Look for redness or swelling around the fistula area. ... This sound may change from a whooshing noise to a whistle-like sound.
Vascular Access for Hemodialysis - Department of Surgery
surgery.ucsf.edu conditions--procedures vascular-ac...
The patient does not need anesthesia for this procedure. ... A vascular surgeon performs AV graft surgery, much like AV fistula surgery, in an outpatient center or ...
Frequently Asked Questions about Dialysis Access Surgery ...
www.bidmc.org transplant-institute frequently-aske...
Dialysis access surgery creates the vascular opening so a needle can be inserted for ... fluid and to correct electrolytes like potassium, sodium, phosphate and calcium, to name a few. ... Where are AV fistulas located and how long do they last?
Fistula and Graft Placement (Eric K. Peden, MD) - YouTube
www.youtube.com watch
Mar 28, 2016 — ... Bootcamp 2015 August 14 - 16, 2015 "Dialysis Access" Fistula and Graft Placement (Eric K. Peden, MD) DICET@Houstonmethodist.org.

this vide shows how to setup an use the SphygmoCor System

Mysterious things happen in nature, and extraordinary birth delivery facts amaze and astound us. And "The baby who didn't know he was born" is one of them; the reason was because his mother didn't break water, so the little one thought was still in the womb. Of course, the amniotic sac was later broken by the doctor, and as soon as this happened the baby began to breath and cry.

LIZ: The first time the doctor made my tip too narrow and I didnt look like myself. The second time the doctor made my tip too wide, and actually took out (removed) extra bone from the side of my nose. That didnt need to be taken out (removed)
My initial consultation with Dr. Nassif was fantastic! He treated me liker his own daughter, and was very caring and thorough. He went over everything!
DR. NASSIF: Liz came into me for a revision rhinoplasty. She told me that shes had two previous rhinoplasties. She was unhappy with the way her nose appeared on her face. She felt it was asymmetric, the tip was kind of bulbous, or large appearing, especially when she looked up, this view, it was very asymmetric. And so, her whole goal was to make it look better, hopefully make it her LAST surgery, and also to help with her breathing.
One of the things thats very important about revision rhinoplasty that you always have to consider is; What are you going to find in there? Even though you can feel the nose, you can palpate it, you can look at it, and you can guess what the other doctors have performed; your first up-hill battle is to see how much scar tissue youre going to be able to identify with. So when you have to open up the nose, you have to remove the scar tissue, identify it: whats there, whats present, whats been removed. Then after you do that, and you have cartilage now ready for grafting, or fascia, or perichondrium, you have to start rebuilding it. Rebuilding it (cartilage) is the second big stage after weve already carved everything; weve carved the cartilage. In that scenario when Im playing with the nose, in regards to staring at the profile, staring at the front of the nose, I go back and forth and look inside and outside of the nose to make sure its as symmetric as possible. That takes a long time One of Lizs main complaints was that on her profile, that her tip stuck out too far. And so one of the things I had to do in surgery is called a medial cura tuck-up, I had to push the tip back, by pushing the tip back, it can make the tip look a little bit wider. But in this situation, I was able to bring everything in as much as I can. After Im finished with everything, and Im happy, then we go ahead and we start to close the nose. Thats putting every little small stitch in perfectly, so that the scar will be minimally visible.
There are four major blood groups determined by the presence or absence of two antigens – A and B – on the surface of red blood cells: Group A – has only the A antigen on red cells (and B antibody in the plasma) Group B – has only the B antigen on red cells (and A antibody in the plasma) Group AB – has both A and B antigens on red cells (but neither A nor B antibody in the plasma) Group O – has neither A nor B antigens on red cells (but both A and B antibody are in the plasma)
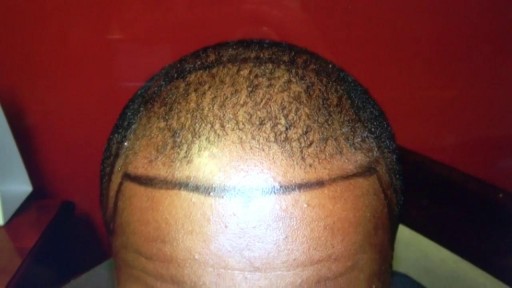
on bald hair loss man at 408-356-8600 by Dr. Diep with photos, of middle eastern man, Asian, Caucasian, Hispanic & Black, most advance hair treatment, treating male pattern baldness, bald head hair loss, receding hairline.
