- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
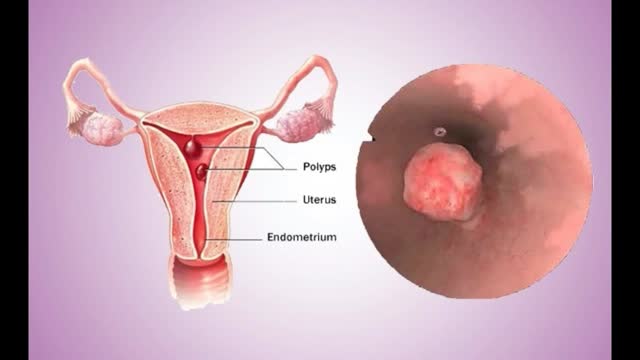
Uterine polyps are growths attached to the inner wall of the uterus that extend into the uterine cavity. Overgrowth of cells in the lining of the uterus (endometrium) leads to the formation of uterine polyps, also known as endometrial polyps. These polyps are usually noncancerous (benign), although some can be cancerous or can eventually turn into cancer (precancerous polyps). Uterine polyps range in size from a few millimeters — no larger than a sesame seed — to several centimeters — golf-ball-size or larger. They attach to the uterine wall by a large base or a thin stalk.

A man's age matters. As men get older, the chances of conceiving and having a healthy child decline. Male fertility starts to decline after 40 when sperm quality decreases. This means it takes longer for their partners to conceive and when they do, there's an increased risk of miscarriage.
Ovarian dermoid cyst and mature cystic ovarian teratoma are terms often used interchangeably to refer to the most common ovarian neoplasm. These slow-growing tumours contain elements from multiple germ cell layers and are best assessed with ultrasound.


From our beginnings in 1990 in primary healthcare, Healthway Medical has grown to become a respected medical group in Singapore. With over 100 clinics and medical centres, Healthway Medical has a wide network of medical centres and clinics in Singapore.
We offer comprehensive services including GP & family medicine clinics, health screening, adult specialists, baby & child specialists, dental services and allied healthcare services.

Although it demands an advanced set of skills that remain substantially hard to do, many of the salient steps of “open” surgery, including suturing, are credibly “replicated” in its laparoscopic counterpart with the intention of achieving similar optimal results. This video demonstrates how to tie Laparoscopic Roeder's Knot. Laparoscopic Roeder's Knot is one of the oldest knots used in laparoscopic surgery. It is used most commonly during laparoscopic appendectomy surgery. Recent literature, though abundant with numerous reports pertaining to a variety of endoscopic knotting techniques and technologies, appears to lack scientific data but Roeder's knot is a time tasted extracorporeal slip knot that is secure for 6-8 mm diameter tubular structure.
For more information please contact:
World Laparoscopy Hospital
Cyber City, Gurugram, NCR DELHI
INDIA 122002
Phone & WhatsApp: +919811416838, + 91 9999677788
Get the best medical animation videos made at https://www.b2w.tv/healthcare-video-production
Check out more animated healthcare videos from out blog here https://www.b2w.tv/blog/health....care-marketing-video
Medical device manufacturers need to find new and innovative ways to explain their products to potential buyers.
It can be difficult for potential buyers to understand how a medical device works, and even more difficult to visualize how it would be used in a clinical setting.
Medical animation videos are the perfect way to showcase your medical devices.
They are engaging, easy to understand, and help potential buyers see how your product would fit into their workflow.
Jump to the video you like:
8. Pharming Healthcare 0:09
7. ThermoFisher Scientific 2:46
6. Fibrogen 5:49
5. OrthAlign 9:29
4. Edwards LifeSciences 11:34
3. Edwards LifeSciences 12:51
2. Edwards LifeSciences 13:43
1. Edwards LifeSciences 18:14
Check out more Healthcare Videos we have made for our clients:
1. Healthcare Explainer Video for WelbeHealth: https://on.b2w.tv/3OFRaWo
2. Healthcare Product Explainer Video for Edwards Lifesciences: https://on.b2w.tv/3OSdMDb
3. Healthcare Commercial Video for Coopervision: https://on.b2w.tv/45muvpf
4. Healthcare Marketing Video for OrthAlign: https://on.b2w.tv/3P8KBgD
5. Healthcare Video Marketing with The Video-First Approach: https://on.b2w.tv/3LiNDfW
6. 12 Best Brand Archetypes for Healthcare Videos: https://on.b2w.tv/3EIQ0Vu
Want to learn more about Healthcare Videos? Check out our blogs:
1. 10 Best Healthcare Marketing Videos: https://on.b2w.tv/47LxhpJ
2. 5 Animated Healthcare Commercial Videos: https://on.b2w.tv/47IgpAd
3. 11 Animated Healthcare Explainer Videos: https://on.b2w.tv/3Zd7fYM
4. How Long Does It Take To Make an Healthcare Explainer Video: https://on.b2w.tv/45nasak
5. Script for Healthcare Explainer Videos: https://on.b2w.tv/47IY1af
6. Guide to Making Your Own Healthcare Explainer Video: https://on.b2w.tv/3P6FKMR
#medicaldevice #medicalanimation #medicalanimations

A giant abdominal wall hernia can develop from an existing ventral or incisional hernia, sometimes arising after one or more failed repair attempts. These hernias may also result from a traumatic injury where the abdomen was required to be left open and healing was delayed. In giant abdominal wall hernias, multiple loops of intestines and sometimes other abdominal organs reside within the hernia sac. The abdominal wall muscles then become conditioned to this and retract reducing the available space inside the abdomen.

This Unorthodox Procedure Makes Short People A Foot Taller

Blood clotting, or coagulation, is an important process that prevents excessive bleeding when a blood vessel is injured. Platelets (a type of blood cell) and proteins in your plasma (the liquid part of blood) work together to stop the bleeding by forming a clot over the injury.
In developing countries, domestic animals (eg, dogs) are common sources of infection. In the United States, bats and wild animals (eg, raccoons) are the most common reservoirs of infection. The acquisition of rabies from bats can occur from an unrecognized bite or a scratch, and possibly by inhalation of aerosolized viral particles. Bats are found in all states except Hawaii, and spelunking (cave exploration) is a risk factor for rabies acquisition from bats.
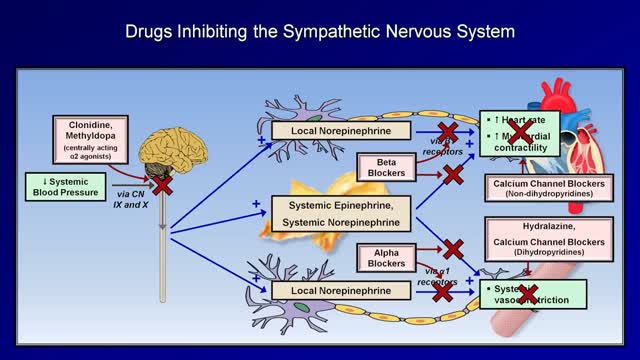
Medications to treat high blood pressure Thiazide diuretics. ... Beta blockers. ... Angiotensin-converting enzyme (ACE) inhibitors. ... Angiotensin II receptor blockers (ARBs). ... Calcium channel blockers. ... Renin inhibitors

Knee pain location can often tell you what type of knee pain you have. If you confirm that with common symptoms and what aggravates it… you can get a pretty good idea of ‘why my knee hurts’. So, here’s a quick look at the most common type of knee problems.
‘The 3 Essential Exercises EVERYONE Should Do’ … Watch this EXCLUSIVE video, only here: https://stefan-becker.mykajabi.com/3-essentials
QUESTIONS? I answer questions here now: I’ve started a Facebook Group to help people achieve their musculo-skeletal goals. Join here… https://www.facebook.com/groups/bodyfixexercises
AND I’m developing a Coaching Program! Over 12 weeks, I help people with posture related issues—like neck, shoulder, & upper back pain—discover their root problem and correct it using science-backed mobilising, stretching, & strengthening exercises… so they can feel straight, strong, flexible, & pain free again (and get back to doing what they love). Find out more, and join the wait list here… https://stefan-becker.mykajabi.com/waiting-list
0:00 Intro
0:11 Pain at the front of the knee (Pain in kneecap)
0:42 Pain below kneecap
1:40 Pain on inside of knee
3:05 Pain below knee on inside
3:29 Pain on outside of knee
3:28 Pain above knee
3:28 Pain behind knee
---------------------------------------
Mentioned in this video...
How To Fix Pain In The Front Of The Knee… (Runner's Knee) https://youtu.be/g0qmx_0enAA
Looking to stop your knee problems? Do this...
Knee Strengthening Exercises To Prevent Knee Pain
https://youtu.be/Pk-ae_lyx7M
How To Treat Patellar Tendinopathy (Jumper’s Knee) & Quadriceps Tendinopathy
https://youtu.be/MkPwsb-rQwU
---------------------------------------
If you’re asking yourself ‘what’s the cause of my knee pain?’ or ‘what kind of knee pain do I have?’ (so that you can look up solutions to your knee pain on YouTube) the position of your knee pain will tell you a lot.
THE MOST COMMON KNEE PAIN TYPES?
Knee pain during running (or actually kneecap pain while running) is usually just that… Runner’s Knee (PATELLOFEMORAL PAIN SYNDROME, or it’s old name: Chondromalacia Patella) If you get knee pain while cycling it will often be the same thing. Same with knee pain with stairs.
Knee pain while squatting could be Runner’s Knee, but if you get pain in the tendon below the kneecap, it’s more likely to be Patellar Tendonitis or Jumper’s Knee.
Meniscus Tears will give you pain on the inside of the knee that is a localised pain, can feel as if it gets stuck, or feel like it’s going to give way, and often it’s hard to fully straighten or fully bend your knee.
Knee pain on the outside of the knee is usually Iliotibial Band Syndrome
ALSO COVERED:
Infrapatellar Fat Pad Syndrome (Hoffa's Syndrome)
Osgood-Schlatter Disease
Medial Collateral Ligament Tear
Iliotibial Band Syndrome
Osteoarthritic Knee Pain
Pes Anserine Bursitis.
Quadriceps Tendinopathy
Popliteus Strain
Baker’s Cyst
ACL Or PCL Tear/Rupture
------------------------------------
#bodyfixexercises #kneepainrelief #kneepain

Hemodialysis is a process that uses a membrane (dialyzer) to: Remove wastes, such as urea, from the blood. Restore the proper balance of electrolytes in the blood. Eliminate extra fluid from the body.

Syphilis is a highly contagious disease spread primarily by sexual activity, including oral and anal sex. Occasionally, the disease can be passed to another person through prolonged kissing or close bodily contact. Although this disease is spread from sores, the vast majority of those sores go unrecognized. The infected person is often unaware of the disease and unknowingly passes it on to his or her sexual partner. Pregnant women with the disease can spread it to their baby. This disease, called congenital syphilis, can cause abnormalities or even death to the child. Syphilis cannot be spread by toilet seats, door knobs, swimming pools, hot tubs, bath tubs, shared clothing, or eating utensils.

A spinal cord injury is not the sort of thing you have to wonder about having. If you've suffered a spinal cord injury, your life is in danger, and you'll know you're injured. You can't use symptoms to diagnose the sort of spinal cord injury you have, and every patient's prognosis is different. Some make a miraculous recovery within months; others need years of physical therapy and still make little to no progress.
Pleurisy is a condition in which the pleura — a membrane consisting of a layer of tissue that lines the inner side of the chest cavity and a layer of tissue that surrounds the lungs — becomes inflamed. Also called pleuritis, pleurisy causes sharp chest pain (pleuritic pain) that worsens during breathing. A variety of underlying conditions can cause pleurisy. Treatment of pleurisy involves pain control and treating the underlying condition.

Dialysis services at UC San Diego Health: https://health.ucsd.edu/care/kidney/dialysis
UC San Diego Health Licensed Clinical Social Worker, Norma Reggev, discusses hemodialysis as a treatment option for failing kidneys with patient testimonials. Discussion includes In Center Hemodialysis and Home Hemodialysis.
0:00 - Hemodialysis
1:34 - When Should Dialysis Begin?
2:00 - What is Dialysis?
2:25 - How Hemodialysis Works
3:15 - In-Center Hemodialysis Considerations
3:42 - Patient Shares Their Experience With In-Center Hemodialysis
7:30 - Home Hemodialysis Considerations
8:35 - Patient Shares Their Experience With Home Hemodialysis
12:23 - Types of Vascular Access

The superior vena cava is a major vein in a person's body. It carries blood from the head, neck, upper chest, and arms to the heart. Superior vena cava syndrome (SVCS) occurs when a person's superior vena cava is partially blocked or compressed. Cancer is usually the main cause of SVCS.
Magnetic Resonance Imaging (MRI) "sees" inside the body by mapping the position of water molecules, which exist at different densities in different types of tissue. Watch the video above for a sample of some impressive MRI images of the human body in action.
