- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
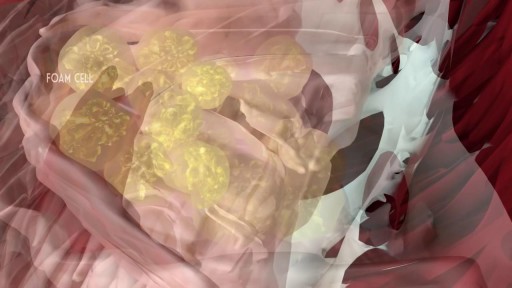
Atherosclerosis is a process in which blood, fats such as cholesterol, and other substances build up on your artery walls. Eventually, deposits called plaques may form. The deposits may narrow — or block — your arteries. These plaques can also rupture, causing a blood clot.
In developing countries, domestic animals (eg, dogs) are common sources of infection. In the United States, bats and wild animals (eg, raccoons) are the most common reservoirs of infection. The acquisition of rabies from bats can occur from an unrecognized bite or a scratch, and possibly by inhalation of aerosolized viral particles. Bats are found in all states except Hawaii, and spelunking (cave exploration) is a risk factor for rabies acquisition from bats.
Mitral valve regurgitation, known as leaky heart valve, can be treated with the MitraClip procedure, especially if you're not a candidate for surgery. As premier heart specialists in the Rocky Mountains, Aurora Denver Cardiology Associates physicians perform this procedure and believe it can be an essential treatment for heart health.

Repair Deviated Nasal Septum, Endoscopic Septoplasty, endoscopic surgery, Stapler repair of nasal septum, Dr B. Todd Schaeffer.

This Unorthodox Procedure Makes Short People A Foot Taller

Syphilis is a highly contagious disease spread primarily by sexual activity, including oral and anal sex. Occasionally, the disease can be passed to another person through prolonged kissing or close bodily contact. Although this disease is spread from sores, the vast majority of those sores go unrecognized. The infected person is often unaware of the disease and unknowingly passes it on to his or her sexual partner. Pregnant women with the disease can spread it to their baby. This disease, called congenital syphilis, can cause abnormalities or even death to the child. Syphilis cannot be spread by toilet seats, door knobs, swimming pools, hot tubs, bath tubs, shared clothing, or eating utensils.

Body Restorations will do an “Early Assessment” when you come in for physiotherapy; this allows therapists to identify the more complicated cases quickly and get started with treatment right away. If you are feeling pain now, it is best that you seek treatment as soon as possible. Research has proven that people who seek treatment for their pain immediately have less of a chance of it becoming an issue later own. Early intervention is always the best option. Visit - https://stalbertphysiotherapy.com/contact/

Hemodialysis is a process that uses a membrane (dialyzer) to: Remove wastes, such as urea, from the blood. Restore the proper balance of electrolytes in the blood. Eliminate extra fluid from the body.
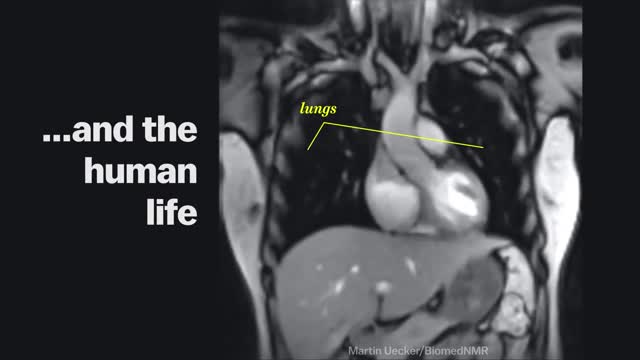
Magnetic Resonance Imaging (MRI) "sees" inside the body by mapping the position of water molecules, which exist at different densities in different types of tissue. Watch the video above for a sample of some impressive MRI images of the human body in action.

A coma is a prolonged state of unconsciousness. During a coma, a person is unresponsive to his or her environment. The person is alive and looks like he or she is sleeping. However, unlike in a deep sleep, the person cannot be awakened by any stimulation, including pain.

Blood clotting, or coagulation, is an important process that prevents excessive bleeding when a blood vessel is injured. Platelets (a type of blood cell) and proteins in your plasma (the liquid part of blood) work together to stop the bleeding by forming a clot over the injury.

In this video I discuss sexual function for people with a spinal cord injury. The amount of feeling and function can vary drastically depending on the level and severity of the injury to the spinal cord.

A spinal cord injury is not the sort of thing you have to wonder about having. If you've suffered a spinal cord injury, your life is in danger, and you'll know you're injured. You can't use symptoms to diagnose the sort of spinal cord injury you have, and every patient's prognosis is different. Some make a miraculous recovery within months; others need years of physical therapy and still make little to no progress.
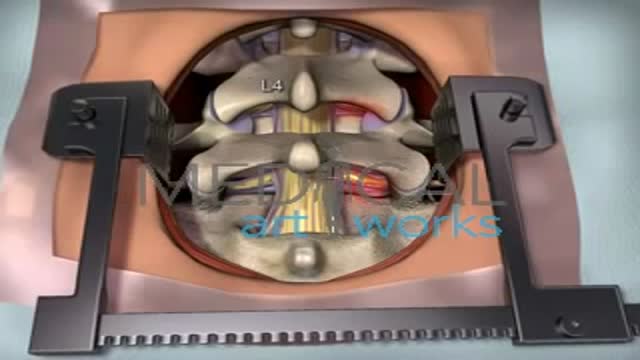
The goal of a decompression surgery is usually to relieve pain caused by nerve root pinching. There are two common causes of lumbar nerve root pressure: from a lumbar herniated disc or lumbar spinal stenosis. This type of pain is usually referred to as a radiculopathy, or sciatica. A decompression surgery involves removing a small portion of the bone over the nerve root and/or disc material from under the nerve root to relieve pinching of the nerve and provide more room for the nerve to heal. The most common types of decompression surgery are microdiscectomy and laminectomy.

Ganglion cysts are the most common mass or lump in the hand. They are not cancerous and, in most cases, are harmless. They occur in various locations, but most frequently develop on the back of the wrist. These fluid-filled cysts can quickly appear, disappear, and change size.

The superior vena cava is a major vein in a person's body. It carries blood from the head, neck, upper chest, and arms to the heart. Superior vena cava syndrome (SVCS) occurs when a person's superior vena cava is partially blocked or compressed. Cancer is usually the main cause of SVCS.
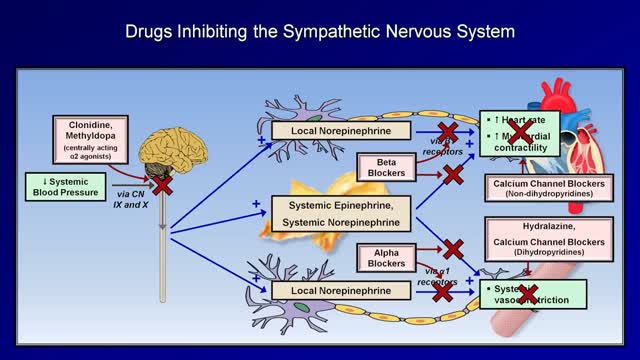
Medications to treat high blood pressure Thiazide diuretics. ... Beta blockers. ... Angiotensin-converting enzyme (ACE) inhibitors. ... Angiotensin II receptor blockers (ARBs). ... Calcium channel blockers. ... Renin inhibitors

Dialysis services at UC San Diego Health: https://health.ucsd.edu/care/kidney/dialysis
UC San Diego Health Licensed Clinical Social Worker, Norma Reggev, discusses hemodialysis as a treatment option for failing kidneys with patient testimonials. Discussion includes In Center Hemodialysis and Home Hemodialysis.
0:00 - Hemodialysis
1:34 - When Should Dialysis Begin?
2:00 - What is Dialysis?
2:25 - How Hemodialysis Works
3:15 - In-Center Hemodialysis Considerations
3:42 - Patient Shares Their Experience With In-Center Hemodialysis
7:30 - Home Hemodialysis Considerations
8:35 - Patient Shares Their Experience With Home Hemodialysis
12:23 - Types of Vascular Access

Today, we're going to expand on our past postural work and exercises. We have taken a look at a few variations of this exercise. The next progression is to move into standing against the wall. This exercise hits many different spots including your pecs and mid-back. The key is to breathe and work on it slowly. Stick with it and you'll make some change! Check us out on Social Media! Facebook: https://www.facebook.com/striveptandperformance/ Instagram: https://www.instagram.com/striveptandperf/ Twitter: https://twitter.com/StrivePTandPerf Blog: http://www.strivept.ca/blog
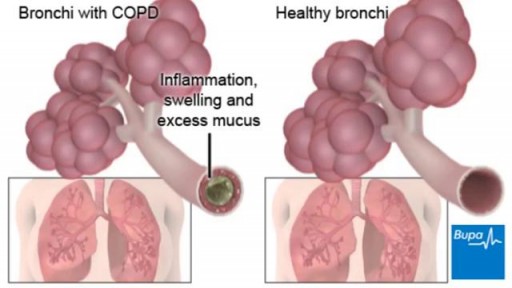
COPD (chronic obstructive pulmonary disease) makes it hard for you to breathe. The two main types are chronic bronchitis and emphysema. The main cause of COPD is long-term exposure to substances that irritate and damage the lungs. This is usually cigarette smoke. Air pollution, chemical fumes, or dust can also cause it. At first, COPD may cause no symptoms or only mild symptoms. As the disease gets worse, symptoms usually become more severe. They include A cough that produces a lot of mucus Shortness of breath, especially with physical activity Wheezing Chest tightness Doctors use lung function tests, imaging tests, and blood tests to diagnose COPD. There is no cure. Treatments may relieve symptoms. They include medicines, oxygen therapy, surgery, or a lung transplant. Quitting smoking is the most important step you can take to treat COPD.
