- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Needle fasciotomy (aponeurotomy) is usually a 15-Minute in-office procedure for Dupuytren's contracture. Performed under local anesthesia, in the office, by board-certified plastic surgeon Reza Momeni, MD. This is a minimally invasive treatment for Dupuytren's.

Stay active and push your body to its limit – tips on how you can mend strained muscles and prevent injury.
The key difference between monophasic and biphasic defibrillator is that the monophasic defibrillator is a type of defibrillation waveform where a shock is delivered to the heart from one vector as shown below. Whereas, in biphasic defibrillation, shock is delivered to the heart via two vectors.

Ganglion cysts are the most common mass or lump in the hand. They are not cancerous and, in most cases, are harmless. They occur in various locations, but most frequently develop on the back of the wrist. These fluid-filled cysts can quickly appear, disappear, and change size.

Watch that video of the 10 Worst Plastic Surgery Failures
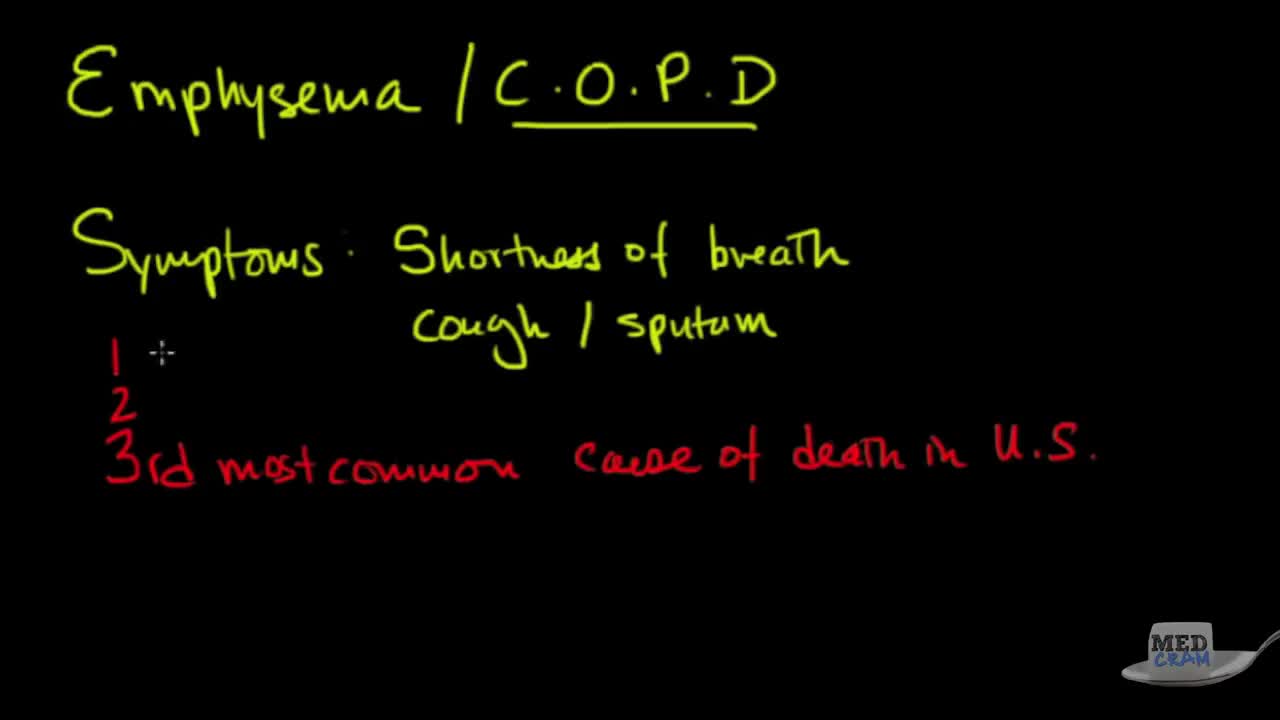
Emphysema, also known as COPD, is a chronic condition with multiple factors that impact survival and life expectancy. Stages of COPD are generally defined using the GOLD criteria (Global Initiative for Chronic Obstructive Lung Disease). It has four levels or stages: mild - or Stage 1.
Histology of Dense Regular Connective Tissue
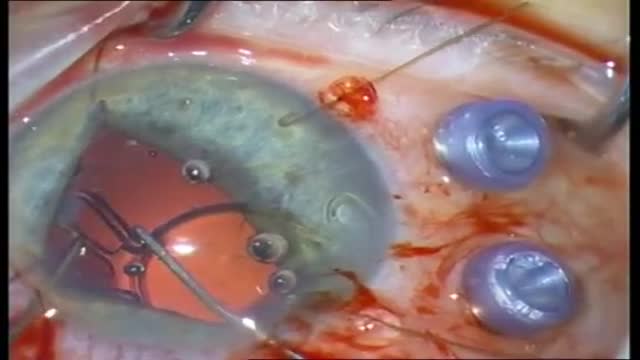
Patients with candida endophthalmitis who have chorioretinitis with vitreal involvement should be treated with vitrectomy and systemic antifungal therapy with amphotericin B (Choice B) and/or fluconazole. An early vitrectomy improves the likelihood of a positive outcome, and intravitreal injection of amphotericin B may be of help. Prompt diagnosis and treatment of candida endophthalmitis is essential, as the condition can worsen quickly.

Signs Of Heart Attack In Women, Healthy Habits, What To Do When Someone Is Having A Stroke.--- http://grow-younger-blood.good-info.co --- High Blood Pressure Cured In 9 Minutes Is it possible to drop your high blood pressure below 120/80 in just 9 minutes? Unbelievable…but the answer is YES! Not only is it possible…thousands of people have done it already. In fact, this little technique has become the #1 “underground” high blood pressure trend of the year. And we’re expecting it to become mainstream very soon. What’s more…this method requires NO pills, supplements, diets, or strenuous workouts. I explain this all here in today’s video… http://grow-younger-blood.good-info.co

Amanda walks Chelsea through how to do the basics of a one leg squat, as she tries not to fall over. Do it at home, at work, or at the gym! No equipment needed! Check us out on Social Media! Facebook: https://www.facebook.com/striveptandperformance/ Instagram: https://www.instagram.com/striveptandperf/ Twitter: https://twitter.com/StrivePTandPerf Blog: http://www.strivept.ca/blog
New York Plastic Surgery ,Dr. Robert Vitolo ,board certified plastic surgeon , brings you into the operating room for a glimpse at how his transumbilical breast augmentation procedure is performed. Dr. Vitolo, a pioneer in the 'no visible scar' breast enlargement surgery, has been using this technique since 1994. Dr. Vitolo use Allergan Natrelle saline breast implants and Mentor saline implants. Dr. Vitolo also performs a removal of silicone gel implants and replacement with saline implants using the transumbilical method.
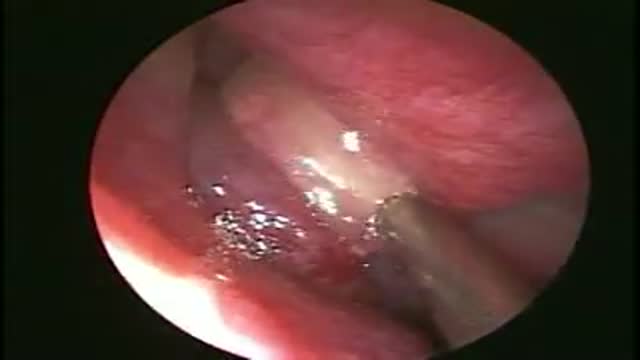
Drainage of a maxillary Sinus pyocoele
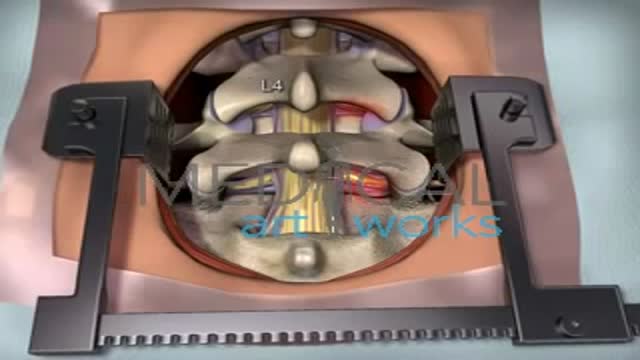
The goal of a decompression surgery is usually to relieve pain caused by nerve root pinching. There are two common causes of lumbar nerve root pressure: from a lumbar herniated disc or lumbar spinal stenosis. This type of pain is usually referred to as a radiculopathy, or sciatica. A decompression surgery involves removing a small portion of the bone over the nerve root and/or disc material from under the nerve root to relieve pinching of the nerve and provide more room for the nerve to heal. The most common types of decompression surgery are microdiscectomy and laminectomy.
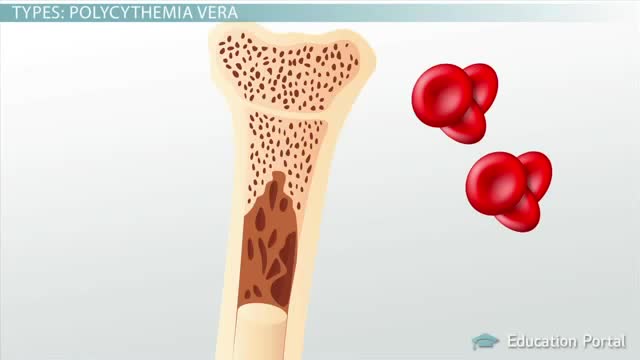
Polycythemia vera (pol-e-sigh-THEE-me-uh VEER-uh) is a slow-growing type of blood cancer in which your bone marrow makes too many red blood cells. Polycythemia vera may also result in production of too many of the other types of blood cells — white blood cells and platelets. These excess cells thicken your blood and cause complications, such as such as a risk of blood clots or bleeding. Polycythemia vera isn't common. It usually develops slowly, and you may have it for years without noticing signs or symptoms. Often, polycythemia vera is found during a blood test done for some other reason. Without treatment, polycythemia vera can be life-threatening. However, with proper medical care, many people experience few problems related to this disease. Over time, there's a risk of progressing to more-serious blood cancers, such as myelofibrosis or acute leukemia.
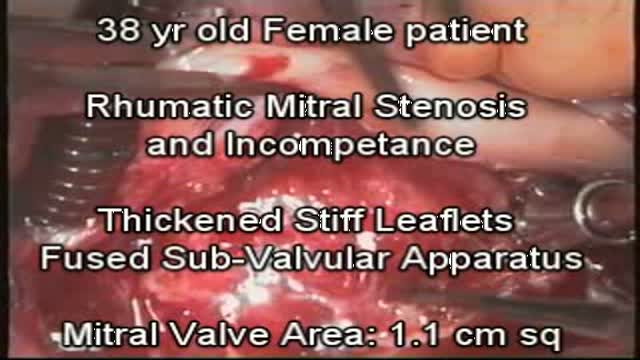
Rhumatic fever has almost been eraicated in the developed world, however it remains prevelent in many under developed countries and causes devastating damage to heart valves. Up till recently valve replacement was the treatment of choice. The long term results and sequelae of valve replacement are...
common knowledge. Mitral and tricuspid valve replacement results are on the whole far worse than for example Aortic valve. Mitral valve replacement should be the last resort and patients with very severe valvular and sub valvular mitral disease can nowadays be helped by mitral valve repair. NO MITRAL OR TRICUSPID VALVE SHOULD BE REPLACED IF IT CAN BE REPAIRED

LIZ: The first time the doctor made my tip too narrow and I didnt look like myself. The second time the doctor made my tip too wide, and actually took out (removed) extra bone from the side of my nose. That didnt need to be taken out (removed)
My initial consultation with Dr. Nassif was fantastic! He treated me liker his own daughter, and was very caring and thorough. He went over everything!
DR. NASSIF: Liz came into me for a revision rhinoplasty. She told me that shes had two previous rhinoplasties. She was unhappy with the way her nose appeared on her face. She felt it was asymmetric, the tip was kind of bulbous, or large appearing, especially when she looked up, this view, it was very asymmetric. And so, her whole goal was to make it look better, hopefully make it her LAST surgery, and also to help with her breathing.
One of the things thats very important about revision rhinoplasty that you always have to consider is; What are you going to find in there? Even though you can feel the nose, you can palpate it, you can look at it, and you can guess what the other doctors have performed; your first up-hill battle is to see how much scar tissue youre going to be able to identify with. So when you have to open up the nose, you have to remove the scar tissue, identify it: whats there, whats present, whats been removed. Then after you do that, and you have cartilage now ready for grafting, or fascia, or perichondrium, you have to start rebuilding it. Rebuilding it (cartilage) is the second big stage after weve already carved everything; weve carved the cartilage. In that scenario when Im playing with the nose, in regards to staring at the profile, staring at the front of the nose, I go back and forth and look inside and outside of the nose to make sure its as symmetric as possible. That takes a long time One of Lizs main complaints was that on her profile, that her tip stuck out too far. And so one of the things I had to do in surgery is called a medial cura tuck-up, I had to push the tip back, by pushing the tip back, it can make the tip look a little bit wider. But in this situation, I was able to bring everything in as much as I can. After Im finished with everything, and Im happy, then we go ahead and we start to close the nose. Thats putting every little small stitch in perfectly, so that the scar will be minimally visible.
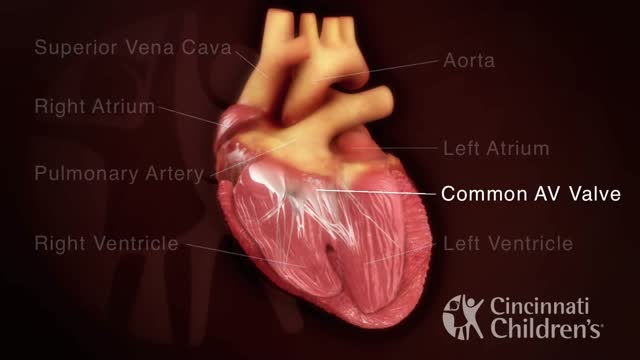
An atrioventricular septal defect (AVSD) is a heart defect in which there are holes between the chambers of the right and left sides of the heart, and the valves that control the flow of blood between these chambers may not be formed correctly. This condition is also called atrioventricular canal (AV canal) defect or endocardial cushion defect. In AVSD, blood flows where it normally should not go. The blood may also have a lower than normal amount of oxygen, and extra blood can flow to the lungs. This extra blood being pumped into the lungs forces the heart and lungs to work hard and may lead to

Placenta accreta is the most common accounting for approximately 75% of all cases. Placenta Increta occurs when the placenta attaches even deeper into the uterine wall and does penetrate into the uterine muscle.

Watch that video of Female Genital Infection Causes and Symptoms

Hemodialysis is a process that uses a membrane (dialyzer) to: Remove wastes, such as urea, from the blood. Restore the proper balance of electrolytes in the blood. Eliminate extra fluid from the body.
