- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
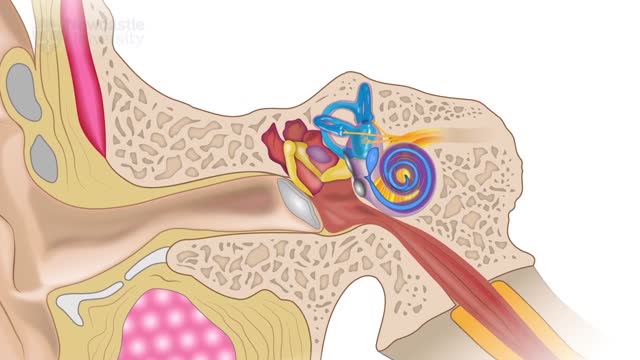
Dizziness is a word that is often used to describe two different feelings. It is important to know exactly what you mean when you say "I feel dizzy," because it can help you and your doctor narrow down the list of possible problems. Lightheadedness is a feeling that you are about to faint or "pass out." Although you may feel dizzy, you do not feel as though you or your surroundings are moving. Lightheadedness often goes away or improves when you lie down. If lightheadedness gets worse, it can lead to a feeling of almost fainting or a fainting spell (syncope). You may sometimes feel nauseated or vomit when you are lightheaded. Vertigo is a feeling that you or your surroundings are moving when there is no actual movement. You may feel as though you are off balance, spinning, whirling, falling, or tilting. When you have severe vertigo, you may feel very nauseated or vomit. You may have trouble walking or standing, and you may lose your balance and fall.
In human anatomy, the radial artery is the main blood vessel, with oxygenated blood, of the lateral aspect of the forearm.

If you could stand in someone else's shoes...Hear what they hear See what they see Feel what they fell Would you treat them differently?

Skin cancer is the most common of all cancer types, accounting for an estimated one third of all new cases. It’s important to take the right steps to ensure proper protection and adopt good sun care habits no matter what your age or stage in life.

Get our Knee Resilience Program here: https://store.e3rehab.com/products/knee-resilience
👟 Vivo Barefoot: Get 15% off all shoes! - https://www.vivobarefoot.com/e3rehab
What is patellofemoral pain, also referred to as runner’s knee? Check out the video to find out!
Want to watch more? Check out our full video: https://youtu.be/K3HxB6rAeDo?t
Subscribe to our channel and turn on notifications so you don't miss any videos: @E3Rehab
We are Doctors of Physical Therapy who specialize in rehabilitation, pain, performance, and injury risk reduction. Our mission is simple: empower YOU to overcome your setbacks and crush your goals using evidence-based education. For more info, check out: https://e3rehab.com/
More videos: https://www.youtube.com/@E3Rehab/videos
Podcast: https://open.spotify.com/show/....5ZbaI145Bk94Guq7olMJ
Instagram: https://www.instagram.com/e3rehab/
Twitter: https://twitter.com/E3Rehab
---
Disclaimer: The information presented is not intended as medical advice or to be a substitute for medical counseling but is intended for entertainment purposes only. If you are experiencing pain, please seek the appropriate healthcare professional.
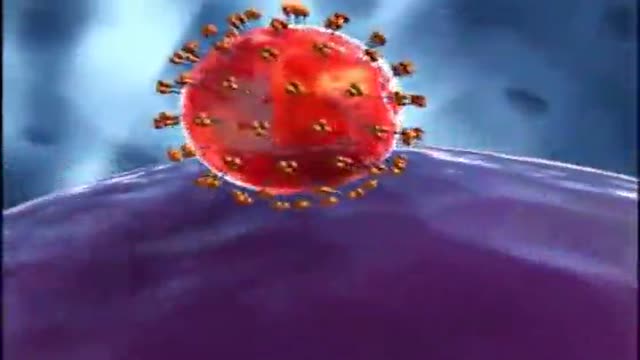
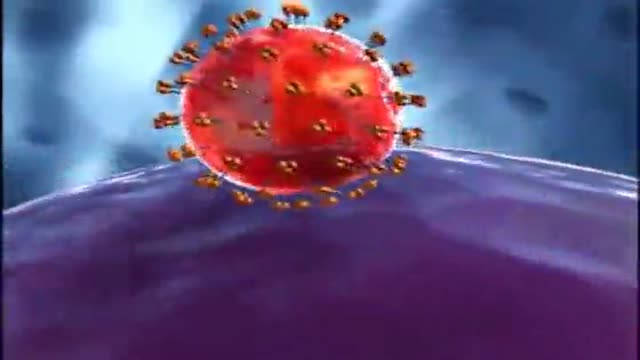
Mechanism of action of a novel HIV drug called Tipranavir
Gleevecs mechanism of Action
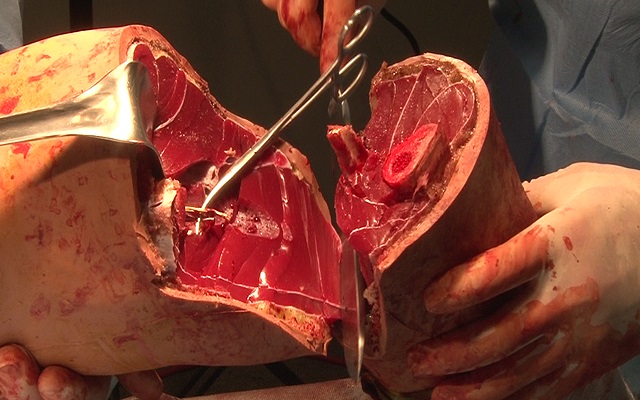
Watch that Above Knee Amputation Surgery video

Anatomy of Back Muscles and Spinal Cord
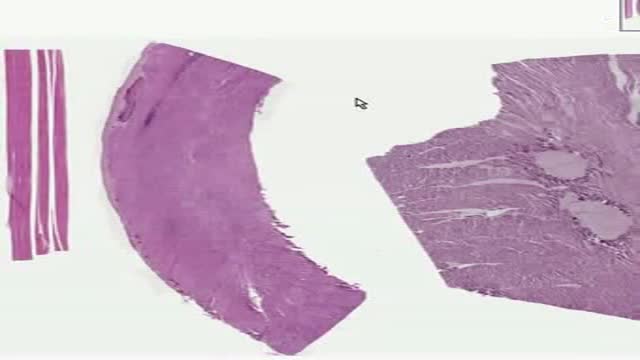
Histology of Mucles Skeletal Smooth Cardiac

Click here to subscribe to Dr. Pimple Popper: https://www.youtube.com/@DrPimplePopper/
Join All Access Memberships here:
https://www.youtube.com/channe....l/UCgrsF4TYwmrV0QsXb
Click here to see my favorite POPS:
Most Popular Pops: https://www.youtube.com/playli....st?list=PLJZ_ok3xiAi
Blackheads: https://www.youtube.com/playli....st?list=PLJZ_ok3xiAi
DPOW’s: https://www.youtube.com/playli....st?list=PLJZ_ok3xiAi
Steatocystomas: https://www.youtube.com/playli....st?list=PLJZ_ok3xiAi
Cysts: https://www.youtube.com/playli....st?list=PLJZ_ok3xiAi
Lipomas: https://www.youtube.com/playli....st?list=PLJZ_ok3xiAi
Soft Pops: https://www.youtube.com/playli....st?list=PLJZ_ok3xiAi
Poppin Off' Show with Dr Pimple Popper: https://youtube.com/playlist?l....ist=PLJZ_ok3xiAi_XPY
__
Connect with Dr. Pimple Popper on Social Media:
Follow Dr. Pimple Popper on Instagram: https://bit.ly/3smTOED
Follow Dr. Pimple Popper on TikTok: https://bit.ly/2MXWDM9
Follow Dr. Pimple Popper on Facebook: https://bit.ly/3oU3Rz7
Follow Dr. Pimple Popper on Twitter: https://bit.ly/2MXWDM9
Follow Dr. Sandra Lee on Instagram: https://bit.ly/2LscBO8
Subscribe to SLMD YouTube to never miss a skincare video:
https://www.youtube.com/@SLMDskincare
More ways to connect with me:
Download the Dr. Pimple Popper All Access App:
https://apps.apple.com/us/app/....dr-pimple-popper/id1
Click here to begin free trial of All-Access: https://allaccess.drpimplepopper.com/
Welcome to the world of Dr. Pimple Popper, the one and only Sandra Lee, MD! As a board certified dermatologist, skin cancer surgeon, and cosmetic surgeon, I am a highly sought-after expert in the field of dermatology.
On this channel, you'll find a treasure trove of videos that offer a window into my world.
Hopefully you'll learn about various skin conditions, hair and nail issues, and cutting-edge cosmetic surgery techniques. Whether you're struggling with blackheads, acne, cysts, warts, or looking for Botox, fillers, or liposuction, you'll find helpful advice and information here.
But this channel isn't just about skin care - it's about the amazing people I encounter every day. You'll get to know some of my incredible patients and their stories, and maybe even fall in love with dermatology just as much as I have!
Disclaimer: This video may contain dermatologic surgical and/or procedural content. The content seen in this video is provided only for medical education purposes and is not intended to be a substitute for professional medical advice, diagnosis, or treatment.
#DrPimplePopper #DrSandraLee #Dermatology #SLMD #Skincare
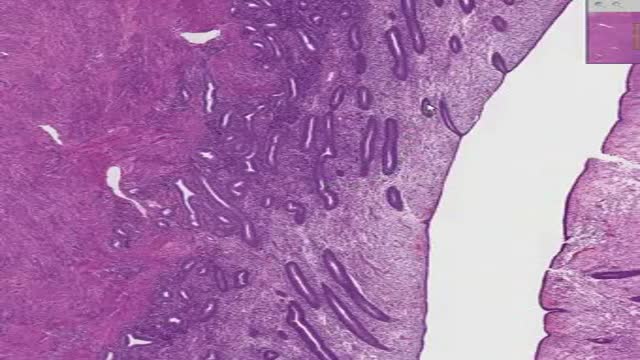
Histology of Proliferative Endometrium

Dr. Rowe shows an easy exercise that can give knee pain relief within seconds.
This exercise will help traction open the knee, relieving pressure and tension. It can be done throughout the day at home, and only requires only a small towel.
Let us know how it works for you!
***************************
Dr. Michael Rowe
St. Joseph, Michigan chiropractor
If you are looking for effective neck, back, or sciatica pain relief, contact us at 269-408-8439 or visit us at https://www.BestSpineCare.com
Facebook: https://www.facebook.com/bestspinecare
Twitter: https://www.twitter.com/stjoechiro
Instagram: https://www.instagram.com/stjoechiro
Your local St. Joseph | Benton Harbor | Stevensville Michigan chiropractor
SpineCare Decompression and Chiropractic Center
3134 Niles Rd
Saint Joseph, MI 49085
**MEDICAL DISCLAIMER**
All information, content, and material of this video or website is for informational and demonstration purposes only. It is not intended to serve as a substitute for the consultation, diagnosis, and/or medical treatment of a qualified physician or healthcare provider.
Don’t use this content as a replacement for treatment and advice given by your doctor or health care provider. Consult with your doctor or healthcare professional before doing anything contained in this content.
By watching this video, you agree to indemnify and hold harmless SpineCare Decompression and Chiropractic Center (and its representatives) for any and all losses, injuries, or damages resulting from any and all claims that arise from your use or misuse of this content. SpineCare Decompression and Chiropractic Center makes no representations about the accuracy or suitability of this content.
USE OF THIS CONTENT IS AT YOUR OWN RISK.
#kneepain #kneepainrelief #kneepainexercise
Epilepsy is a chronic disorder, the hallmark of which is recurrent, unprovoked seizures. Many people with epilepsy have more than one type of seizure and may have other symptoms of neurological problems as well. Sometimes EEG testing, clinical history, family history and outlook are similar among a group of people with epilepsy. In these situations, their condition can be defined as a specific epilepsy syndrome. The human brain is the source of human epilepsy. Although the symptoms of a seizure may affect any part of the body, the electrical events that produce the symptoms occur in the brain. The location of that event, how it spreads and how much of the brain is affected, and how long it lasts all have profound effects. These factors determine the character of a seizure and its impact on the individual. Esssentially, anything the brain can do, it can do in the form of a seizure. Having seizures and epilepsy can affect one's safety, relationships, work, driving and so much more. Public perception and treatment of people with epilepsy are often bigger problems than actual seizures.

Tonsillitis is inflammation of the tonsils, two oval-shaped pads of tissue at the back of the throat — one tonsil on each side. Signs and symptoms of tonsillitis include swollen tonsils, sore throat, difficulty swallowing and tender lymph nodes on the sides of the neck. Most cases of tonsillitis are caused by infection with a common virus, but bacterial infections also may cause tonsillitis. Because appropriate treatment for tonsillitis depends on the cause, it's important to get a prompt and accurate diagnosis. Surgery to remove tonsils, once a common procedure to treat tonsillitis, is usually performed only when bacterial tonsillitis occurs frequently, doesn't respond to other treatments or causes serious complications.
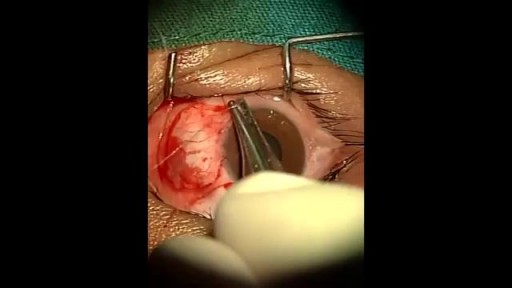
An eye web is a noncancerous, triangular growth that may occur on one or both eyes. It's more common in people who spend a lot of time in the sun, such as those who work outdoors. The painless growth may be slightly raised and contain obvious blood vessels. It may cause irritation and possibly affect vision. Treatment usually isn't necessary. Eyedrops or surgery may help in severe cases.
You may have recently found out that you are deficient or know someone who is. It's shocking for most people when they have never had a problem before and believe nothing has changed to make it a problem now. The truth is that a lot has changed, and vitamin D deficiency and insufficiency is now a global public-health problem affecting an estimated 1 billion people worldwide. The most well-known consequences to not having enough vitamin D are rickets in children and osteomalacia in adults. These are far from the only problems associated with a vitamin D deficiency.

arteriovenous hemodialysis access has been the "gold standard" for patients needing hemodialysis for the past 30 years. Despite the reported advantages of autologous access, the availability of prosthetic graft material, coupled with the challenging dialysis candidate, has led to a trend of primary prosthetic graft dialysis access in the 1980s and 1990s. In recognition of this unfortunate trend, the National Kidney Foundation Dialysis Outcomes Quality Initiative (DOQI) used evidence from published studies and summary articles to generate clinical practice guidelines, emphasizing a shift back to autologous arteriovenous fistula (AVF) as the key to long-term successful hemodialysis.[1,2] These initial guidelines proposed a goal of 50% autologous AVF as the initial access, with a 40% prevalence of autologous access for a given practice or unit.

Giant cell arteritis is an inflammation of the lining of arteries. Most often, it affects the arteries in your head, especially those in your temples. For this reason, giant cell arteritis is sometimes called temporal arteritis. Giant cell arteritis frequently causes headaches, scalp tenderness, jaw pain and vision problems. If left untreated, it can lead to stroke or blindness. Prompt treatment with corticosteroid medications usually relieves symptoms of giant cell arteritis and may prevent loss of vision. You'll likely begin to feel better within days of starting treatment. But even with treatment, relapses are common. You'll need to visit your doctor regularly for checkups and treatment of any side effects from taking corticosteroids.

Video giving an overview of histology, slide preparation, histological stains, and types of microscopy. This video is a part of our Histology Video Course (https://youtube.com/playlist?l....ist=PLnr1l7WuQdDynxT
Specific topics: what is histology, general composition of tissues, histotechnology: how histology slides are prepared, histology stains, immunohistochemistry, light microscopy vs electron microscopy, and pro tips for learning histology
Additional YouTube Content
Anatomy Videos: https://youtube.com/playlist?l....ist=PLnr1l7WuQdDz2dK
Biochemistry videos: https://youtube.com/playlist?l....ist=PLnr1l7WuQdDzCUC
DaVinci Cases Videos: https://youtube.com/playlist?l....ist=PLnr1l7WuQdDyJUl
The DaVinci Hour Podcast: https://youtube.com/playlist?l....ist=PLnr1l7WuQdDwSm9
DaVinci Academy Website: https://www.dviacademy.com/
