- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

Dr. Joanna Chikwe, explains how patients may feel after heart surgery.
Learn more about the Smidt Heart Institute at Cedars-Sinai at https://ceda.rs/3meIA2A
Learn more about Dr. Joanna Chikwe at https://ceda.rs/3ul6I6t
Connect with us:
https://twitter.com/CedarsSinai
https://www.facebook.com/CedarsSinai
https://www.instagram.com/CedarsSinai
Cedars-Sinai is a leader in providing high-quality healthcare encompassing primary care, specialized medicine and research. Since 1902, Cedars-Sinai has evolved to meet the needs of one of the most diverse regions in the nation, setting standards in quality and innovative patient care, research, teaching and community service. Today, Cedars- Sinai is known for its national leadership in transforming healthcare for the benefit of patients. Cedars-Sinai impacts the future of healthcare by developing new approaches to treatment and educating tomorrow’s health professionals. Additionally, Cedars-Sinai demonstrates a commitment to the community through programs that improve the health of its most vulnerable residents.

Infant Cardio-pulmonary Resuscitation
This video show the steps in a total parotidectomy with VII nerve preservation. The patient had a malignant parotid tumor without VII nerve compromise.

Diabetes Complications and Kidney Disease

this video shows how the adult circumcision is easy by the alisklamp

Transurethral resection of the prostate (also known as TURP, plural TURPs and as a transurethral prostatic resection TUPR) is a urological operation. It is used to treat benign prostatic hyperplasia (BPH). As the name indicates, it is performed by visualising the prostate through the urethra and removing tissue by electrocautery or sharp dissection. This is considered the most effective treatment for BPH. This procedure is done with spinal or general anesthetic. A large triple lumen catheter is inserted through the urethra to irrigate and drain the bladder after the surgical procedure is complete. Outcome is considered excellent for 80-90% of BPH patients. Because of bleeding risks associated with the surgery, TURP is not considered safe for many patients with cardiac problems. As with all invasive procedures, the patient should first discuss medications they are taking with their doctor, most especially blood thinners or anticoagulants, such as warfarin (Coumadin), or aspirin. These may need to be discontinued prior to surgery. Postop complications include bleeding (most common), clotting and hyponatremia (due to bladder irrigation).
Additionally, transurethral resection of the prostate is associated with low but important morbidity and mortality.
Watch that video to know the Difference Between White and Clear Sperm


This surgery is usually done while you are under general anesthesia. That means you will be asleep and pain-free. Healthy skin is taken from a place on your body called the donor site. Most people who are having a skin graft have a split-thickness skin graft. This takes the two top layers of skin from the donor site (the epidermis) and the layer under the epidermis (the dermis). The donor site can be any area of the body. Most times, it is an area that is hidden by clothes, such as the buttock or inner thigh. The graft is carefully spread on the bare area where it is being transplanted. It is held in place either by gentle pressure from a well-padded dressing that covers it, or by staples or a few small stitches. The donor-site area is covered with a sterile dressing for 3 to 5 days. People with deeper tissue loss may need a full-thickness skin graft. This requires an entire thickness of skin from the donor site, not just the top two layers. A full-thickness skin graft is a more complicated procedure. Common donor sites for full-thickness skin grafts include the chest wall, back, or abdominal wall.
A talus fracture is a break in one of the bones that forms the ankle. This type of fracture often occurs during a high-energy event, such as a car collision or a high-velocity fall. Because the talus is important for ankle movement, a fracture often results in significant loss of motion and function. In addition, a talus fracture that does not heal properly can lead to serious complications, including chronic pain. For this reason, many talus fractures require surgery.

An African traditional healer performing a brain surgery.

visit https://www.facebook.com/medical.hint
to check the answers

Blood type (or blood group) is determined, in part, by the ABO blood group antigens present on red blood cells. A blood type (also called a blood group) is a classification of blood based on the presence or absence of inherited antigenic substances on the surface of red blood cells (RBCs).
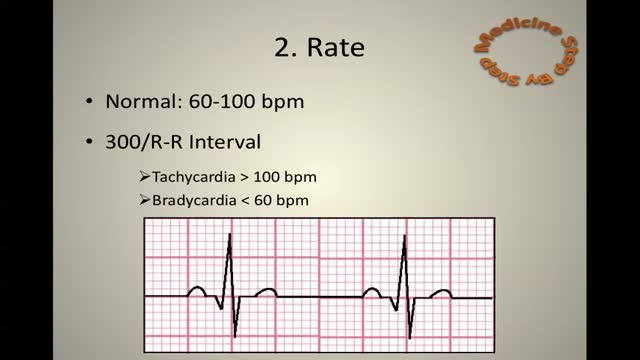
ECG Learn it

Pulmonary edema is almost always treated in the emergency room or hospital. You may need to be in an intensive care unit (ICU). Oxygen is given through a face mask or tiny plastic tubes are placed in the nose. A breathing tube may be placed into the windpipe (trachea) so you can be connected to a breathing machine (ventilator) if you cannot breathe well on your own. The cause of edema should be identified and treated quickly. For example, if a heart attack has caused the condition, it must be treated right away. Medicines that may be used include: Diuretics that remove excess fluid from the body Medicines that strengthen the heart muscle, control the heartbeat, or relieve pressure on the heart
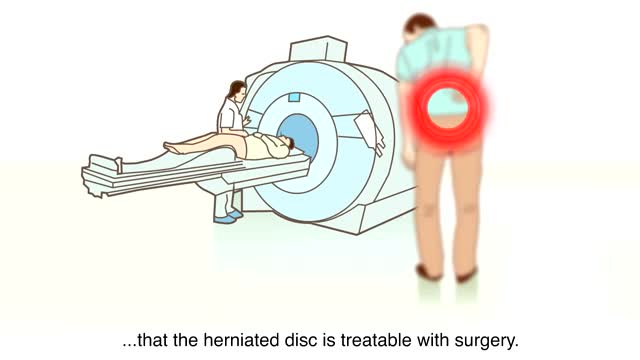
A herniated disk refers to a problem with one of the rubbery cushions (disks) between the individual bones (vertebrae) that stack up to make your spine. A spinal disk is a little like a jelly donut, with a softer center encased within a tougher exterior. Sometimes called a slipped disk or a ruptured disk, a herniated disk occurs when some of the softer "jelly" pushes out through a crack in the tougher exterior. A herniated disk can irritate nearby nerves and result in pain, numbness or weakness in an arm or leg. On the other hand, many people experience no symptoms from a herniated disk. Most people who have a herniated disk don't need surgery to correct the problem.

A cervical rib in humans is an extra rib which arises from the seventh cervical vertebra. Sometimes known as "neck ribs", their presence is a congenital abnormality located above the normal first rib. A cervical rib is estimated to occur in 0.2% (1 in 500 people) to 0.5% of the population.
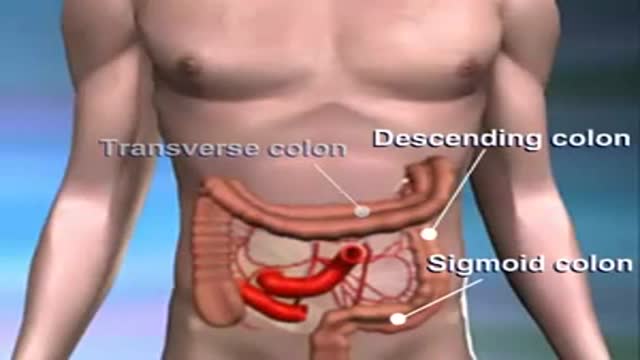
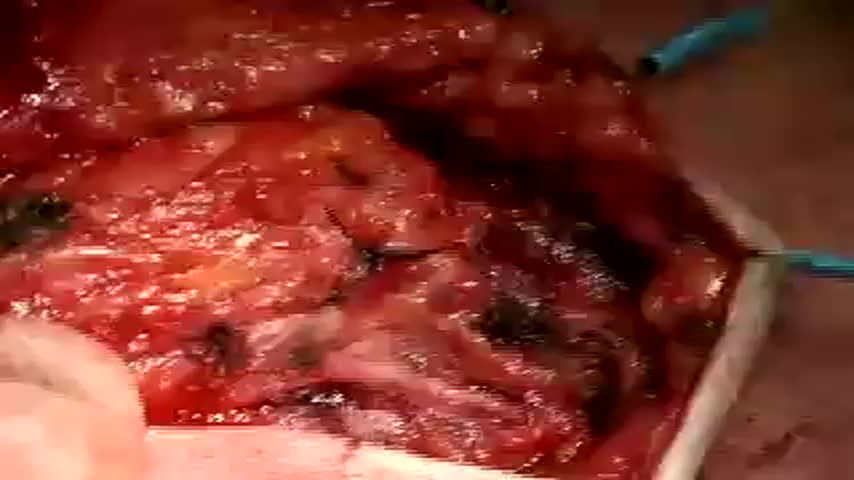
Colon cancer usually begins as a non-cancerous growth. If caught early enough, it can be safely removed with little to no complications.

Dr. Linder is removing a patients breast implants after having five breast augmentations from three previous surgeons. She has baker 4 capsular contracture and is look forward to having them removed. The most common reasons for removing a breast implant include; heath reasons such as back pain, reoccurring complications and the desire for a different shape or size. For implant removal surgery, Dr. Linder makes an inframammary incision (along the breast crease). The implant can be removed intact, or it may need to be punctured before removal. An antibiotic solution is used to irrigate the breast pocket after implant removal. For more information about breast implant removal go to www.implantremoval.net or call Dr. Linder's office at 310-275-4513
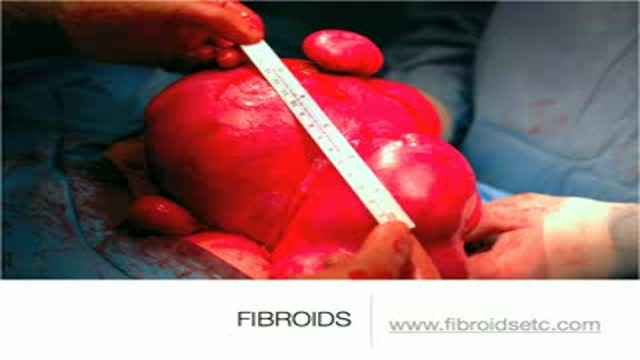
A uterine fibroid (also uterine leiomyoma, myoma, fibromyoma, leiofibromyoma, fibroleiomyoma, and fibroma) (plural of ... myoma is ...myomas or ...myomata) is a benign (non-cancerous) tumor that originates from the smooth muscle layer (myometrium) and the accompanying connective tissue of the uterus. Fibroids are the most common benign tumors in females and typically found during the middle and later reproductive years. While most fibroids are asymptomatic, they can grow and cause heavy and painful menstruation, painful sexual intercourse, and urinary frequency and urgency. Uterine fibroids is the major indication for hysterectomy in the US.[2] Fibroids are often multiple and if the uterus contains too many leiomyomatas to count, it is referred to as uterine leiomyomatosis. The malignant version of a fibroid is uncommon and termed a leiomyosarcoma.
