- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

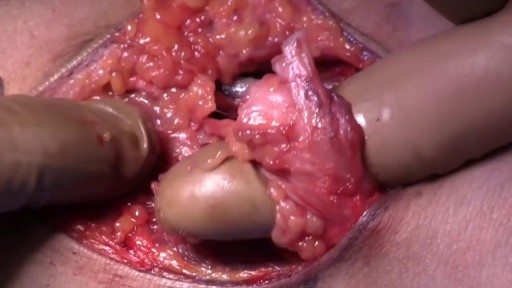
A 28 years old man lost his right arm with a conveyor device in 2014. The video is taken 2 years after replantation. You can see another videos in my site: https://drliaghatclinic.com, https://instagram.com/liaghatclinic, https://t.me/liaghatclinic

mammoplasty, is a surgical enhancement procedure to accentuate the size and shape of a woman’s breasts. While breast augmentation will make the breasts larger, the surgery will not move the breasts closer together or lift sagging breasts. Breast augmentation is tremendous help to patients who desire a fuller profile, who have lost breast volume due to pregnancy or nursing, or who have undergone breast reconstruction and want to gain a more natural look again.
Video is an excellent introduction to Hysterosalpingography and summarizes different pathologies. While the information on this presentation is about health care issues, it is not medical advice. People seeking specific medical advice or assistance should contact their personal physician. Although we believe the information in this presentation to be accurate and timely, because of the rapid advances in health care and our reliance on information provided by outside sources, we make no warranty or guarantee concerning the accuracy or reliability of the content or other material which we may reference. When clinical matters are discussed, the opinions presented are those of the discussants only. The material discussed on the presentation is not intended to present the only or necessarily the best method or procedure, but rather presents the approach or opinion of the discussant. This presentation is provided in an “as is” format without warranties of any kind, expressed or implied, including but not limited to warranties of title, non-infringement or implied warranties of merchantability or fitness for a particular purpose.

Carpal tunnel syndrome is a hand condition that causes numbness, tingling and other symptoms. Carpal tunnel syndrome is caused by a pinched nerve in your wrists A number of factors can contribute to carpal tunnel syndrome, including the anatomy of your wrist, certain underlying health problems and possibly patterns of hand use. Bound by bones and ligaments, the carpal tunnel is a narrow passageway located on the palm side of your wrist. This tunnel protects a main nerve to your hand and the nine tendons that bend your fingers. Compression of the nerve produces the numbness, tingling and, eventually, hand weakness that characterize carpal tunnel syndrome.

Rheumatoid Arthritis,physiology,pathology,clinincal features,manifestations and treatment
Worlds Most Amazing Medical Case
Pelvic ureter. The ureter enters the pelvis, where it crosses anteriorly to the iliac vessels, which usually occurs at the bifurcation of the common iliac artery into the internal and external iliac arteries. Here, the ureters are within 5 cm of one another before they diverge laterally.

Surgical removal of mucocele from lower lip

Terrifying Sinus Infection - Disturbing - Must Watch

ROTIGS medical device by Honolulu inventor Dr. Brad NaPier makes difficult airway intubations easier for medical professionals.
The biceps muscle is located in the front of your upper arm. It is attached to the bones of the shoulder and elbow by tendons — strong cords of fibrous tissue that attach muscles to bones. Tears of the biceps tendon at the elbow are uncommon. They are most often caused by a sudden injury and tend to result in greater arm weakness than injuries to the biceps tendon at the shoulder. Once torn, the biceps tendon at the elbow will not grow back to the bone and heal. Other arm muscles make it possible to bend the elbow fairly well without the biceps tendon. However, they cannot fulfill all the functions of the elbow, especially the motion of rotating the forearm from palm down to palm up. This motion is called supination. To return arm strength to near normal levels, surgery to repair the torn tendon is usually recommended. However, nonsurgical treatment is a reasonable option for patients who may not require full arm function.

Plantar warts are hard, grainy growths that usually appear on the heels or balls of your feet, areas that feel the most pressure. This pressure also may cause plantar warts to grow inward beneath a hard, thick layer of skin (callus). Plantar warts are caused by the human papillomavirus (HPV). The virus enters your body through tiny cuts, breaks or other weak spots on the bottom of your feet. Most plantar warts aren't a serious health concern and may not require treatment. But plantar warts can cause discomfort or pain. If self-care treatments for plantar warts don't work, you may want to see your doctor to have them removed.
intracranial hematoma occurs when a blood vessel ruptures within your brain or between your skull and your brain. The collection of blood (hematoma) compresses your brain tissue. An intracranial hematoma may occur because the fluid that surrounds your brain can't absorb the force of a sudden blow or a quick stop. Then your brain may slide forcefully against the inner wall of your skull and become bruised. Although some head injuries — such as one that causes only a brief lapse of consciousness (concussion) — can be minor, an intracranial hematoma is potentially life-threatening and often requires immediate treatment. An intracranial hematoma often, but not always, requires surgery to remove the blood.
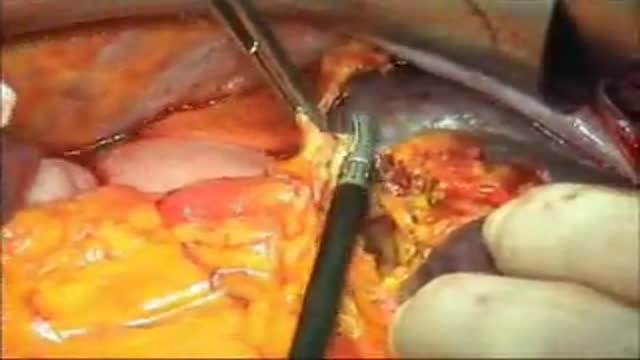
Splenectomy is a surgical procedure that partially or completely removes the spleen.
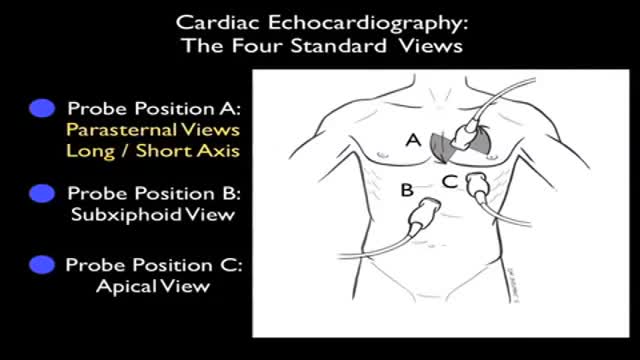
Ultrasound of Heart
The heart itself is made up of 4 chambers, 2 atria and 2 ventricles. De-oxygenated blood returns to the right side of the heart via the venous circulation. It is pumped into the right ventricle and then to the lungs where carbon dioxide is released and oxygen is absorbed. The oxygenated blood then travels back to the left side of the heart into the left atria, then into the left ventricle from where it is pumped into the aorta and arterial circulation.

How do you assess cerebellar function? Ask them to do this as fast as possible while you slowly move your finger. Repeat the test with the other hand. Perform the heel-to-shin test. Have the patient lying down for this and get them to run the heel of one foot down the shin of the other leg, and then to bring the heel back up to the knee and start again.

Carpal Tunnel Syndrome Ergonomics
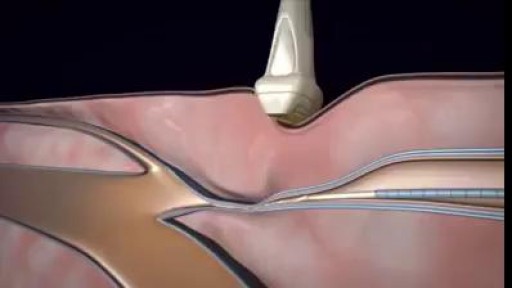
3D animation video of Varicose Veins Sclerotherapy Treatment

Appendicitis is one of the most common surgical problems. One out of every 2,000 people has an appendectomy sometime during their lifetime. Treatment requires an operation to remove the infected appendix. Traditionally, the appendix is removed through an incision in the right lower abdominal wall. In most laparoscopic appendectomies, surgeons operate through 3 small incisions (each ¼ to ½ inch) while watching an enlarged image of the patient’s internal organs on a television monitor. In some cases, one of the small openings may be lengthened to complete the procedure.
