- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos

In this video, we will cover the function of the liver and how cancer may arise.
Non-Hodgkin's lymphoma, also called non-Hodgkin lymphoma, is cancer that originates in your lymphatic system, the disease-fighting network spread throughout your body. In non-Hodgkin's lymphoma, tumors develop from lymphocytes — a type of white blood cell. Non-Hodgkin's lymphoma is more common than the other general type of lymphoma — Hodgkin lymphoma. Many different subtypes of non-Hodgkin's lymphoma exist. The most common non-Hodgkin's lymphoma subtypes include diffuse large B-cell lymphoma and follicular lymphoma.

Mesh repair is based on the anatomical principle with associated complications of a foreign body and recurrence. Use of an un-detached strip of the external oblique aponeurosis in place of mesh between the muscle arch and the inguinal ligament gives a strong and physiologically dynamic posterior wal...l that gives radical cure.
Scott Geller MD of Fort Myers Florida uses A LASAG Yag laser is in thermal mode, 1.5 Joules/pulse to treat the trabecular meshwork between the cornea and iris for glaucoma. The view is of the inside anterior eyeball.

Hypothyroidism and Hyperthyroidism Symptoms: Swollen Neck. A goiter is an enlargement of the thyroid gland. As shown here, an enlarged thyroid can be seen as a swelling in the front of the neck. A goiter can occur with either hypothyroidism or hyperthyroidism

360 tour videos are the latest video marketing trend all industries can be taking advantage of! VR and 360 medical videos, like this one, provide patients with a full understanding of the service. Whether you need a medical VR training video and a VR surgery video or medical videos for students to learn, these healthcare and medical videos will instill trust in your company and services.
Get a quote for your project here: https://epicproductionsllc.com/video-production/
Don't forget to follow us...
Like us on Facebook: https://www.facebook.com/epicproductionsllc/
Follow us on Twitter: https://twitter.com/epicprodllc
Connect with us on LinkedIn: https://www.linkedin.com/compa....ny/epic-productions-
Follow us on Instagram: https://www.instagram.com/epicproductionsllc/

Nose cautery can help prevent nosebleeds. The doctor uses a chemical swab or an electric current to cauterize the inside of the nose. This seals the blood vessels and builds scar tissue to help prevent more bleeding. For this procedure, your doctor made the inside of your nose numb.

Vaginismus Pain Management
Vaginal Hysterectomy utilizing the PlasmaSeal Open Forceps presented by Kristi Keil, MD.
Supraventricular tachycardia (SVT) is an abnormal condition of heart which increases normal heartbeat rate rapidly. Normally, heartbeat rate should be between 80 to 100 beats per minute. For more info: https://goo.gl/14btbU

The examination consists of three portions: Inspection, Palpation, and Synthesis of data from these techniques In addition to palpating for size, also note the gland texture, mobility, tenderness and the presence of nodules. Inspection Inspection: Anterior Approach The patient should be seated or standing in a comfortable position with the neck in a neutral or slightly extended position. Cross-lighting increases shadows, improving the detection of masses. To enhance visualization of the thyroid, you can: Extending the neck, which stretches overlying tissues Have the patient swallow a sip of water, watching for the upward movement of the thyroid gland. quicktime video 251KB video demo from Return to the Bedside Inspection: Lateral Approach After completing anterior inspection of the thyroid, observe the neck from the side. Estimate the smooth, straight contour from the cricoid cartilage to the suprasternal notch. Measure any prominence beyond this imagined contour, using a ruler placed in the area of prominence. Palpation Note: There is no data comparing palpation using the anterior approach to the posterior approach so examiners should use the approach that they find most comfortable. Palpation: Anterior Approach placement of hands for palpatation of thyroid in anterior approach The patient is examined in the seated or standing position. Attempt to locate the thyroid isthmus by palpating between the cricoid cartilage and the suprasternal notch. Use one hand to slightly retract the sternocleidomastoid muscle while using the other to palpate the thyroid. Have the patient swallow a sip of water as you palpate, feeling for the upward movement of the thyroid gland. quicktime video 454KB video demo from Return to the Bedside. Palpation: Posterior Approach placement of hands for palpatation of thyroid in posterior approach The patient is examined in the seated or standing position. Standing behind the patient, attempt to locate the thyroid isthmus by palpating between the cricoid cartilage and the suprasternal notch. Move your hands laterally to try to feel under the sternocleidomstoids for the fullness of the thyroid. Have the patient swallow a sip of water as you palpate, feeling for the upward movement of the thyroid gland.
In this condition, the body retains water instead of excreting it normally in urine. This process upsets the body's balance of minerals called electrolytes, especially sodium. Symptoms can vary depending on how rapidly the condition develops. In some cases, nausea and vomiting, headache, confusion, weakness, and fatigue may be experienced. Treatments include fluid restriction and, possibly, medications to adjust electrolyte balance. Underlying conditions also need treatment.

This cosmetic plastic surgery graphically shows breast implants being removed in an operating room in an actual surgery.
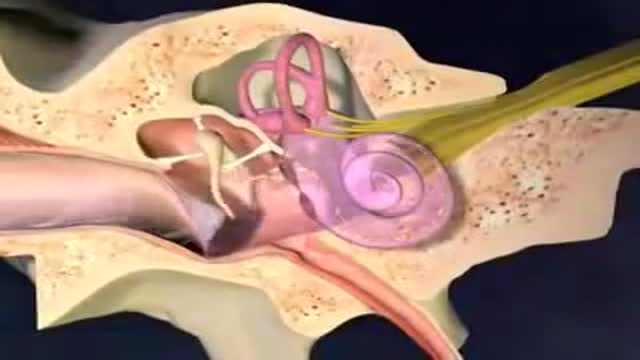
Acute otitis media: Inflammation of the middle ear in which there is fluid in the middle ear accompanied by signs or symptoms of ear infection: a bulging eardrum usually accompanied by pain; or a perforated eardrum, often with drainage of purulent material (pus).

Treatment consists of diet modifications and laxatives A high-fiber diet can be effective, along with over-the-counter medications, such as stool softeners. In some cases, a medical procedure to remove the hemorrhoid may be needed to provide relief.
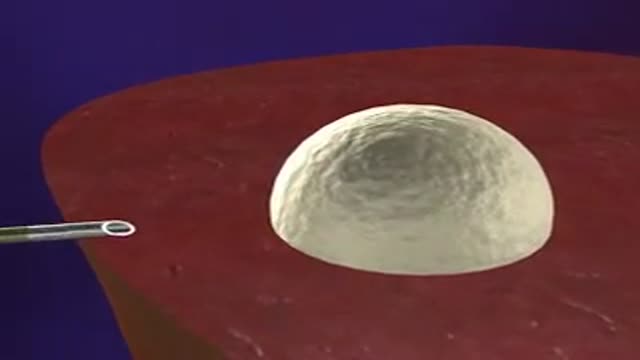
An animation showing the general principle of Radiofrequency Ablation of Hepatocellular carcinoma HCC.
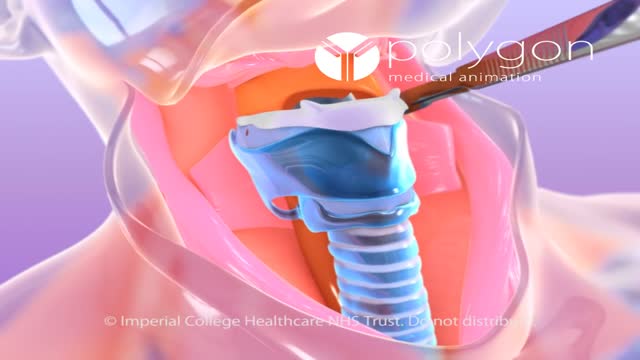
Laryngectomy is the removal of the larynx and separation of the airway from the mouth, nose and esophagus. In a total laryngectomy the entire larynx is removed and in a partial laryngectomy only a portion is taken out. The laryngectomee breathes through an opening in the neck known as a stoma.
Transvenous cardiac pace maker, also called endocardial pacing, is a potentially life saving intervention used primarily to correct profound bradycardia. It can be used to treat symptomatic bradycardias that do not respond to transcutaneous pacing or to drug therapy.
