- Physical Examination
- Surgical Examination
- Ophthalmology
- Clinical Skills
- Orthopedics
- Surgery Videos
- Laparoscopy
- Pediatrics
- Funny Videos
- Cardiothoracic Surgery
- Nursing Videos
- Plastic Surgery
- Otorhinolaryngology
- Histology and Histopathology
- Neurosurgery
- Dermatology
- Pediatric Surgery
- Urology
- Dentistry
- Oncology and Cancers
- Anatomy Videos
- Health and Fitness
- Radiology
- Anaesthesia
- Physical Therapy
- Pharmacology
- Interventional Radiology
- Cardiology
- Endocrinology
- Gynecology
- Emergency Medicine
- Psychiatry and Psychology
- Childbirth Videos
- General Medical Videos
- Nephrology
- Physiology
- Diet and Food Health
- Diabetes Mellitus
- Neurology
- Women Health
- Osteoporosis
- Gastroenterology
- Pulmonology
- Hematology
- Rheumatology
- Toxicology
- Nuclear Medicine
- Infectious Diseases
- Vascular Disease
- Reproductive Health
- Burns and Wound Healing
- Other
Top videos
Sepsis is a potentially life-threatening complication of an infection. Sepsis occurs when chemicals released into the bloodstream to fight the infection trigger inflammatory responses throughout the body. This inflammation can trigger a cascade of changes that can damage multiple organ systems, causing them to fail. If sepsis progresses to septic shock, blood pressure drops dramatically, which may lead to death. Anyone can develop sepsis, but it's most common and most dangerous in older adults or those with weakened immune systems. Early treatment of sepsis, usually with antibiotics and large amounts of intravenous fluids, improves chances for survival. Symptoms & causes Symptoms Many doctors view sepsis as a three-stage syndrome, starting with sepsis and progressing through severe sepsis to septic shock. The goal is to treat sepsis during its early stage, before it becomes more dangerous. Sepsis To be diagnosed with sepsis, you must exhibit at least two of the following symptoms, plus a probable or confirmed infection: Body temperature above 101 F (38.3 C) or below 96.8 F (36 C) Heart rate higher than 90 beats a minute Respiratory rate higher than 20 breaths a minute Severe sepsis Your diagnosis will be upgraded to severe sepsis if you also exhibit at least one of the following signs and symptoms, which indicate an organ may be failing: Significantly decreased urine output Abrupt change in mental status Decrease in platelet count Difficulty breathing Abnormal heart pumping function Abdominal pain Septic shock To be diagnosed with septic shock, you must have the signs and symptoms of severe sepsis — plus extremely low blood pressure that doesn't adequately respond to simple fluid replacement. When to see a doctor Most often sepsis occurs in people who are hospitalized. People in the intensive care unit are especially vulnerable to developing infections, which can then lead to sepsis. If you get an infection or if you develop signs and symptoms of sepsis after surgery, hospitalization or an infection, seek medical care immediately. Causes While any type of infection — bacterial, viral or fungal — can lead to sepsis, the most likely varieties include: Pneumonia Abdominal infection Kidney infection Bloodstream infection (bacteremia) The incidence of sepsis appears to be increasing in the United States. The causes of this increase may include: Aging population. Americans are living longer, which is swelling the ranks of the highest risk age group — people older than 65. Drug-resistant bacteria. Many types of bacteria can resist the effects of antibiotics that once killed them. These antibiotic-resistant bacteria are often the root cause of the infections that trigger sepsis. Weakened immune systems. More Americans are living with weakened immune systems, caused by HIV, cancer treatments or transplant drugs. Risk factors Sepsis is more common and more dangerous if you: Are very young or very old Have a compromised immune system Are already very sick, often in a hospital's intensive care unit Have wounds or injuries, such as burns Have invasive devices, such as intravenous catheters or breathing tubes Complications Sepsis ranges from less to more severe. As sepsis worsens, blood flow to vital organs, such as your brain, heart and kidneys, becomes impaired. Sepsis can also cause blood clots to form in your organs and in your arms, legs, fingers and toes — leading to varying degrees of organ failure and tissue death (gangrene). Most people recover from mild sepsis, but the mortality rate for septic shock is nearly 50 percent. Also, an episode of severe sepsis may place you at higher risk of future infections.
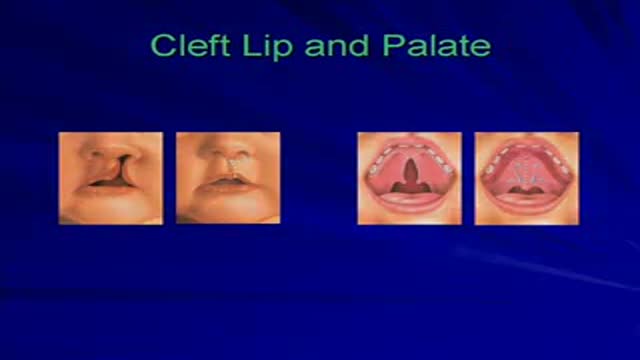
This video is a collection of selected cases of Plastic Surgery performed on children with congenital deformities.
Errata: Cleft Lip Case 2 has a center photo which belongs to case 1 at day of surgery.

Meckels Diverticulum
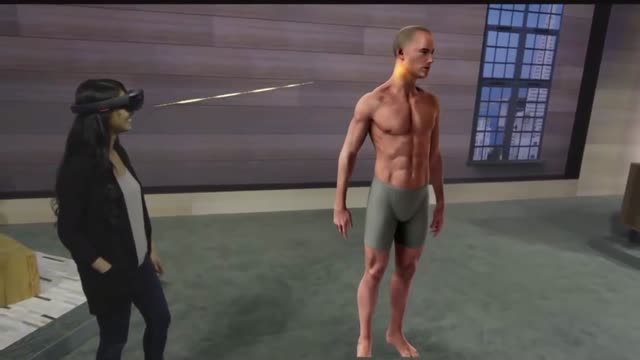
Microsoft HoloLens. Medical Education
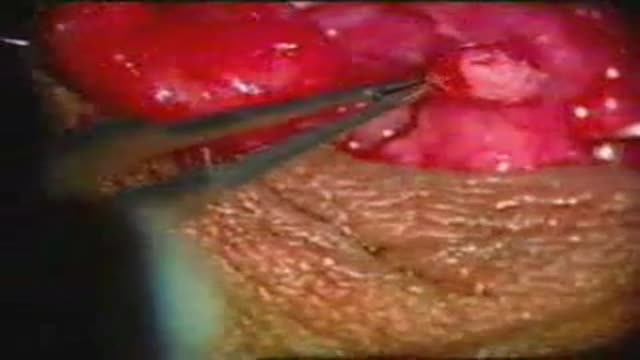
The operation for reversal of vasectomy

Hypothyroidism and Hyperthyroidism Symptoms: Swollen Neck. A goiter is an enlargement of the thyroid gland. As shown here, an enlarged thyroid can be seen as a swelling in the front of the neck. A goiter can occur with either hypothyroidism or hyperthyroidism
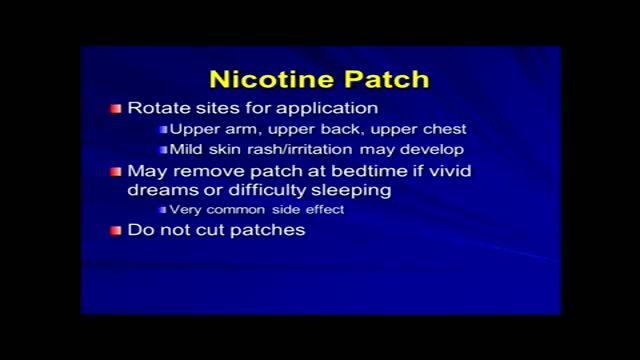
Tobacco use is the most common preventable cause of death. About half of the people who don't quit smoking will die of smoking-related problems. Quitting smoking is important for your health. Soon after you quit, your circulation begins to improve, and your blood pressure starts to return to normal. Your sense of smell and taste return, and it's easier for you to breathe. In the long term, giving up tobacco can help you live longer. Your risk of getting cancer decreases with each year you stay smoke-free. Quitting is not easy. You may have short-term affects such as weight gain, irritability, and anxiety. Some people try several times before they succeed. There are many ways to quit smoking. Some people stop "cold turkey." Others benefit from step-by-step manuals, counseling, or medicines or products that help reduce nicotine addiction. Some people think that switching to e-cigarettes can help you quit smoking, but that has not been proven. Your health care provider can help you find the best way for you to quit.
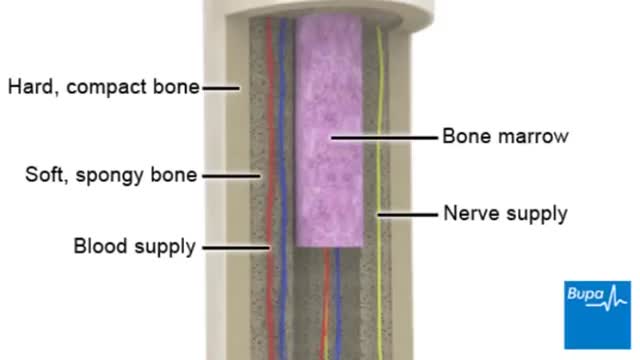
Osteoporosis is a disease in which bones become brittle and fragile due to low bone mass and bone tissue loss. It's the most common type of bone disease, according to the National Institutes of Health (NIH), and increases your risk of fractures, particularly of the hips, spine, and wrists. Prevalence In the United States, nearly 54 million people ages 50 and older were living with osteoporosis or osteopenia (low bone mass ) in 2010, according to a 2014 article in the Journal of Bone and Mineral Research. More specifically, 10.2 million adults had osteoporosis, and 43.4 million adults had osteopenia, which puts a person at high risk for osteoporosis.
In emergencies (eg, asystole), transcutaneous pacing should be tried first. If transvenous pacing is tried, the catheter should be advanced during asynchronous pacing at maximum output until the ventricle has been captured and a palpable pulse is detected in the patient.

360 tour videos are the latest video marketing trend all industries can be taking advantage of! VR and 360 medical videos, like this one, provide patients with a full understanding of the service. Whether you need a medical VR training video and a VR surgery video or medical videos for students to learn, these healthcare and medical videos will instill trust in your company and services.
Get a quote for your project here: https://epicproductionsllc.com/video-production/
Don't forget to follow us...
Like us on Facebook: https://www.facebook.com/epicproductionsllc/
Follow us on Twitter: https://twitter.com/epicprodllc
Connect with us on LinkedIn: https://www.linkedin.com/compa....ny/epic-productions-
Follow us on Instagram: https://www.instagram.com/epicproductionsllc/

Giant cell arteritis is an inflammation of the lining of arteries. Most often, it affects the arteries in your head, especially those in your temples. For this reason, giant cell arteritis is sometimes called temporal arteritis. Giant cell arteritis frequently causes headaches, scalp tenderness, jaw pain and vision problems. If left untreated, it can lead to stroke or blindness. Prompt treatment with corticosteroid medications usually relieves symptoms of giant cell arteritis and may prevent loss of vision. You'll likely begin to feel better within days of starting treatment. But even with treatment, relapses are common. You'll need to visit your doctor regularly for checkups and treatment of any side effects from taking corticosteroids.
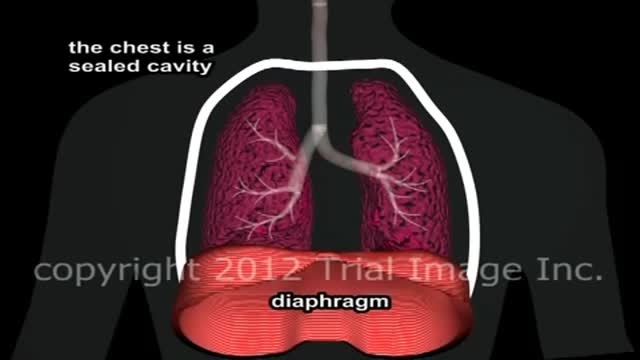
Pulmonary edema Email this page to a friend Email this page to a friend Facebook Twitter Google+ Pulmonary edema is an abnormal buildup of fluid in the lungs. This buildup of fluid leads to shortness of breath. Causes Pulmonary edema is often caused by congestive heart failure. When the heart is not able to pump efficiently, blood can back up into the veins that take blood through the lungs. As the pressure in these blood vessels increases, fluid is pushed into the air spaces (alveoli) in the lungs. This fluid reduces normal oxygen movement through the lungs. These two factors combine to cause shortness of breath.

Anatomy of Back Muscles and Spinal Cord

The bilateral sagittal split osteotomy is an indispensable tool in the correction of dentofacial abnormalities. The technique has been in practice since the late 1800s, but did not reach widespread acceptance and use until several modifications were described in the 1960s and 1970s. Those modifications came from a desire to make the procedure safer, more reliable, and more predictable with less relapse. Those goals continue to stimulate innovation in the field today and have helped the procedure evolve to be a very dependable, consistent method of correction of many types of malocclusion. The operative surgeon should be well versed in the history, anatomy, technical aspects, and complications of the bilateral sagittal split osteotomy to fully understand the procedure and to counsel the patient.
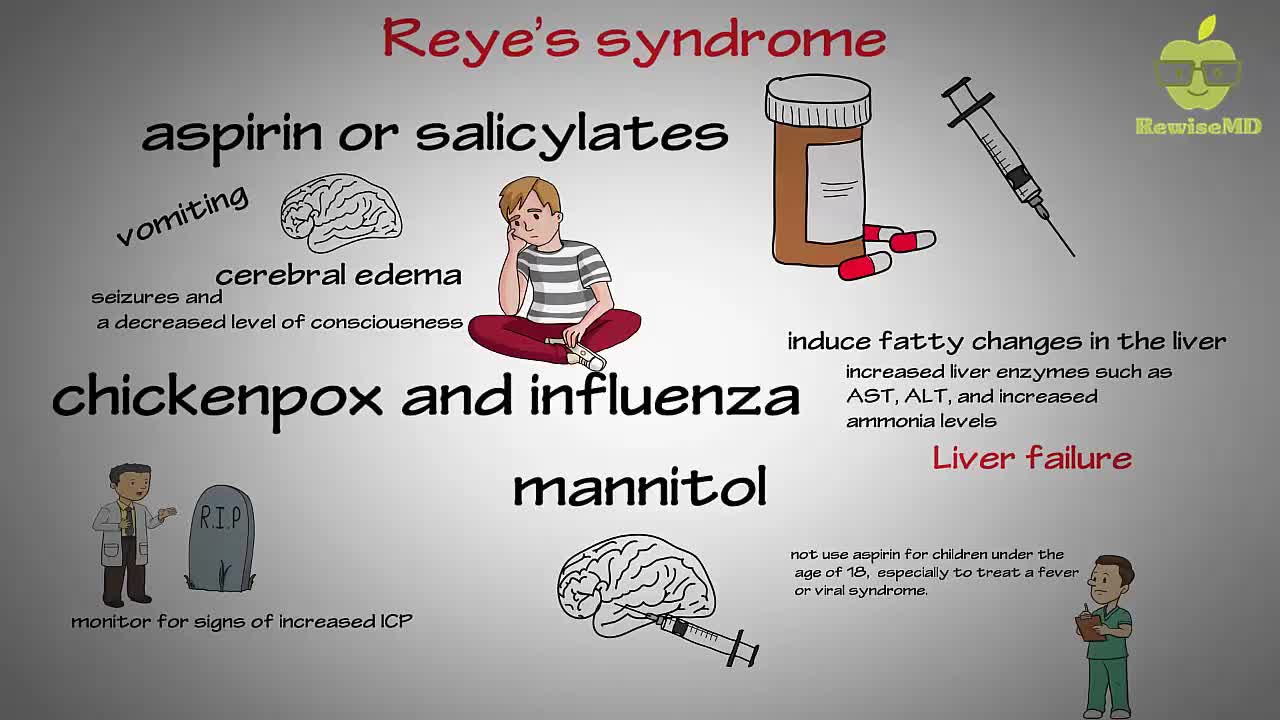
In Reye's syndrome, a child's blood sugar level typically drops while the levels of ammonia and acidity in his or her blood rise. At the same time, the liver may swell and develop fatty deposits. Swelling may also occur in the brain, which can cause seizures, convulsions or loss of consciousness. The signs and symptoms of Reye's syndrome typically appear about three to five days after the onset of a viral infection, such as the flu (influenza) or chickenpox, or an upper respiratory infection, such as a cold
Menorrhagia is the medical term for menstrual periods with abnormally heavy or prolonged bleeding. Although heavy menstrual bleeding is a common concern, most women don't experience blood loss severe enough to be defined as menorrhagia.

Ellis demonstrates the need to drop the tip of the needle when withdrawing medication from a vial.
#NCLEX #NewGrad #ClinicalSkills #HESI #Kaplan #ATI #NursingSchool #NursingStudent #Nurse #RN #PN #Education #LPN #NurseEducator #lvn
🚨 Reminder: shipping deadlines are looming 👀
🎁 Regular Shipping: Order by Friday, December 15
🚀 Expedited Shipping: Order by Monday, December 18
🔍 Still searching for last-minute gifts? Consider a Level Up RN Gift Card! 💌 It’s not only a thoughtful present but also the perfect way to share treasures like Pharmacology Flashcards OR digital treasures like Flashables Digital Nursing Flashcards & the Level Up RN membership. Give the gift of knowledge this holiday season! 🧠⚡️💖 bit.ly/LevelUpRNGC
🚪 Access our Cram Courses, Quizzes and Videos all in one ad free space with Level Up RN Membership https://bit.ly/LevelUpRNMembership
Want more ways to MASTER Clinical Skills? Check out our flashcards & videos!
👇👇👇👇👇👇👇👇👇👇
👉 https://bit.ly/clinicalnursingskills 👈
☝️👆☝️👆☝️👆☝️👆☝️👆
This is your one-stop-shop for materials to help you LEARN & REVIEW so you can PASS Nursing School.
🤔🤔🤔 DO YOU WANT TO PASS your classes, proctored exams and the NCLEX? 🤔🤔🤔 Our resources are the best you can buy. They are built with a single goal: help you pass with no fluff. Everything you need, and nothing you don’t. Don’t take our word for it, though! Check out our hundreds of ⭐️⭐️⭐️⭐️⭐️ reviews from nurses who passed their exams and the NCLEX with Level Up RN.
🗂️ Our Ultimate Nursing School Survival kit is your number 1 resource to get through nursing school and to pass the NCLEX. Whether you're just starting school or you’re already prepping for the NCLEX, this bundle of flashcards is the best you can buy. It covers all the information you need to know to pass all your exams and it has FREE shipping!
➡️ https://bit.ly/TUNSSK ⬅️
L👀king for EVEN MORE resources to survive Nursing School? Make your Nursing School experience your own! Life’s difficult enough—learning shouldn’t be.
🪅 Games https://nursesquad.com
💻 Digital resources https://bit.ly/NursingStudyCourses
📅 Organizational tools https://bit.ly/OrganizingSchool
✨Want perks? Join our channel!
https://youtube.com/leveluprn/join
🏷 Head to https://leveluprn.com/specials for all our latest deals!🥳️
📧 LOOKING FOR FREE RESOURCES TO HELP WITH YOUR EXAMS? Get exclusive tips, latest video releases and more delivered to your email!
➡️ https://leveluprn.com/signup ⬅️
⚕ 👩 LEVEL UP NURSE SQUAD 👩⚕️
All of the nurses at Level Up RN are here to help! Cathy Parkes started helping her fellow classmates back when she was in nursing school, tutoring so they could pass their exams and graduate. After she got her BSN and started working as an RN at Scripps Encinitas Hospital, she started this YouTube channel to help nursing students around the world. Since then she has built a team of top-notch dedicated nurses and nurse educators who are focused on improving nursing education and supporting career advancement for nurses everywhere. With flashcards, videos, courses, organizational tools and more, we are singularly focused on helping students and nurses Level Up on their exams and nursing careers.
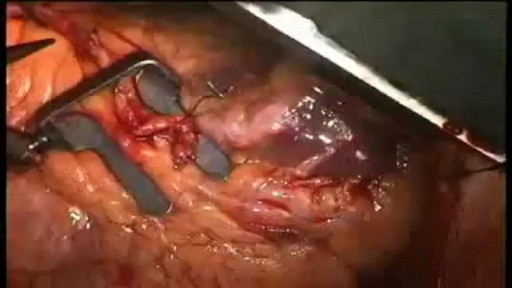
Mesh repair is based on the anatomical principle with associated complications of a foreign body and recurrence. Use of an un-detached strip of the external oblique aponeurosis in place of mesh between the muscle arch and the inguinal ligament gives a strong and physiologically dynamic posterior wal...l that gives radical cure.
When your arteries cannot supply enough blood to your heart, your doctor may recommend coronary artery bypass graft (CABG) surgery. One of the most common heart surgeries in the United States, CABG surgery restores blood flow to your heart. Approximately every 10 minutes, someone has beating heart or "off-pump" bypass surgery1. Beating heart bypass surgery is — in simple terms — bypass surgery that is performed on your heart while it is beating. Your heart will not be stopped during surgery. You will not need a heart-lung machine. Your heart and lungs will continue to perform during your surgery. Surgeons use a tissue stabilization system to immobilize the area of the heart where they need to work. Beating heart bypass surgery is also called Off Pump Coronary Artery Bypass Surgery (OPCAB). Both OPCAB and conventional on-pump surgery restore blood flow to the heart. However, off-pump bypass surgery has proven to reduce side effects in certain types of patients.
